![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!IXc-!,w_120,h_120,c_fill,f_webp,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F9f7142a0-6602-495d-ab65-0e4c98cc67d4_450x450.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!lBsj!,e_trim:10:white/e_trim:10:transparent/h_48,c_limit,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F0e0f61bc-e3f5-4f03-9c6e-5ca5da1fa095_1848x352.png)
Signals From [Clinical Trials] - Part 02: The Plan
14 Signals Across Speed, Simplicity, Cost, Setup, & Recruitment

Welcome back to Signals From [Space], the place to discover what's next in healthcare technology— and who’s building it — one [space] at a time. I’m a founder and patient navigating the noisy, complex world of healthtech and sharing what I learn along the way.
"Research is formalized curiosity. It is poking and prying with a purpose."
Introduction
In Part 1 of this series we introduced the clinical trials landscape, including why trials exist, who’s involved, and how study phases are structured to bring safe, effective drugs and devices to market. But we also learned just how hard that journey can be to complete — only 10% of Phase I drugs go on to receive FDA approval.1 E Pluribus Unum, remember? Out of many, one.
In the spirit of Zora Neale Hurston, today’s Curiosity Expedition pokes and pries into the first stages of clinical research. My aim with this article is to explore what happens behind the scenes before the first patient volunteers arrive. We hear so much about the FDA approvals and pivotal trials poised to transform medicine, but much less about the decades-long efforts that make these headlines and realities possible.

Today we zoom-in to the first stage in our clinical trial journey. These are the promising signs of progress in the pre-clinical phase: discovery, study design, site selection and recruitment. We know from Part 1 that these also happen to be a few of our greatest headwinds and challenges in this space. So without further ado, let’s explore 14 Signals of a better tomorrow in clinical trials, fueled by improvements in speed, simplicity, cost, setup, and recruitment.
Signals
Speed
Q: How do we get new drugs and devices to study sites faster?
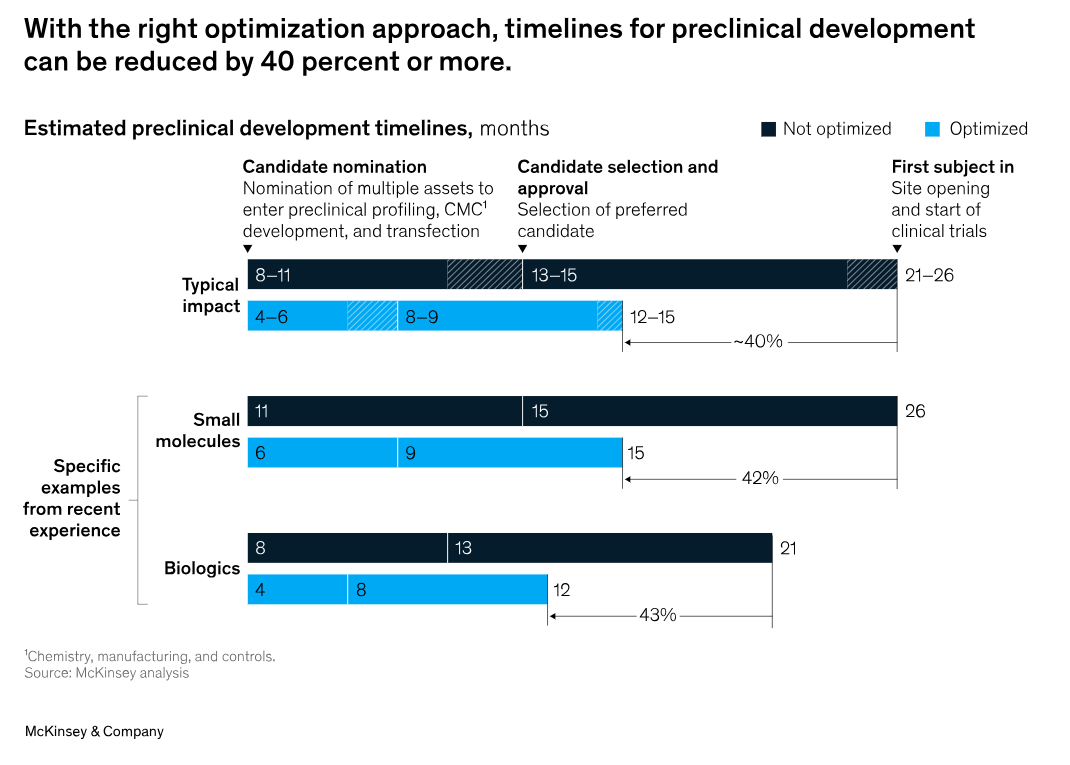
SIGNAL 01. Reducing preclinical development time
It takes about 24 months for new drug candidates to reach the first patient volunteers, and about 60 months for medical devices to do the same.23
A McKinsey report published earlier this year suggests pharma companies can reduce the time they take to reach first-in-human (FIH) studies by 40 percent or more, with drugs progressing from candidate nomination to the start of clinical trials in as little as 12 to 15 months.4 By front-loading investments and running some processes in parallel, where possible, companies can rethink design and risk profiles to get to revenues faster and extend exclusivity in the market. Like any great product learning to scale, it comes down to learning which parts of the the process can be standardized and replicated for future use.
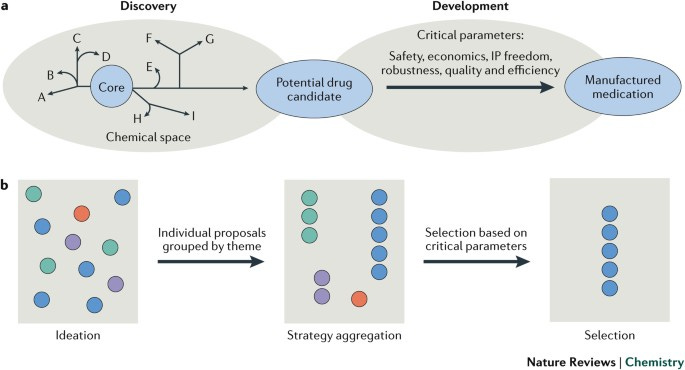
SIGNAL 02. Streamlining candidate nomination & approval
Identifying promising drug candidates and securing the necessary regulatory approvals is a slow and resource-intensive process, often extending drug development timelines.
Accelerating this process could yield significant financial benefits, with potential gains exceeding $400 million for a pharma company advancing 3 to 5 new drugs into studies each year.5
At its core, identifying candidates is about chemistry. The overall goal of a pharma chemistry team is to identify and develop a commercially viable approach to a drug candidate. But routinely delivering innovation across the drug development lifecycle requires more than great chemistry— it demands significant organizational focus and strategic selection.6 Clearly, the economic benefits can make the internal efforts worthwhile.
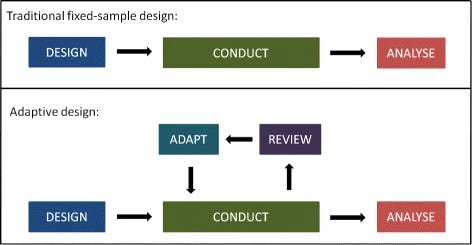
SIGNAL 03. Enhancing trial flexibility with adaptive designs
Traditional clinical trial designs can be rigid and time-consuming, which makes it harder for researchers to make real-time adjustments in response to emerging data, potentially slowing down the development process.
Adaptive trial designs have emerged in response to the shortcomings of randomized clinical trials. RCTs have a few inherent qualities that make them more challenging to pull off, including the need for large sample sizes, long study durations, and high costs to name a few. Adaptive designs aim to address all these barriers. A 2016 review article published in NEJM shares 4 case studies where adaptive designs were used to illustrate benefits, limitations, and considerations for a successful trial.7
Types of adaptive designs include:
Seamless Phase 2-3 Designs (e.g. INHANCE Trial)
Sample-size Re-estimations (e.g. CHAMPION PHOENIX Trial)
Group Sequential Designs (e.g. EXAMINE trial)
Population-enrichment Designs (e.g. Biomarker-driven designs)
Simplicity
Q: How might we simplify complex clinical trial designs & processes?
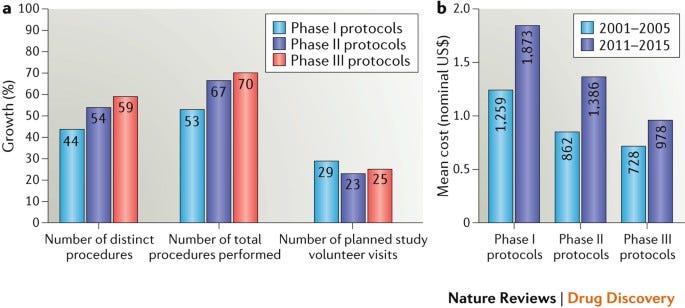
SIGNAL 04. Simplifying complex study protocols
Trials have grown in complexity with significant cost and time implications. Complexity can be quantified in several ways including the number of (a) sites; (b) geographies; (c) eligibility criteria; (d) patients; (e) clinical procedures; (f) and data points.
One study evaluating over 100 trial protocols reported that the median number of clinical trial procedures grew by 57% over a decade (non-device clinical trials).8 More complex protocols can expand study times and contribute to slow recruitment, poor retention, and an increase in the number of protocol amendments. Another review of over 3,000 studies (non-device) reported that nearly 60% of the protocols resulted in one or more protocol amendments, adding time and cost to the study. One-third of the overall amendment changes were rated by the sponsors to be somewhat or completely avoidable.9
SIGNAL 05. Managing data overload
There is an inverse relationship between the complexity in a protocol and performance and quality of the clinical trial.
An increased burden in data monitoring is a direct result of more data collection and complexity of trials. It has been reported that nearly 90% of non-core data points are verified by site monitors, adding substantial time and costs to the study even though the data are not utilized to support key objectives of the program (e.g., regulatory approval decision making, reimbursement).10
SIGNAL 06. Addressing protocol delays
An estimated 85% of all clinical trials will experience delays, with 94% delayed by over a month.11
The financial impact can be massive, costing between $600,000 - $8 million every day. A Nature analysis examining the causes of clinical trial delays found that strategic problems, commercial barriers, and operational issues were to blame in almost a quarter of all trials.12
Cost
Q: How do we manage (or reverse) the trend of rising study costs?
SIGNAL 07. Managing high development costs
Clinical trials comprise the largest portion of overall medical device development costs.13
For complex medical devices that require a Premarket Application (PMA) submission to FDA, clinical trial costs account for between 50 to 60 percent of total R&D expenditures.14
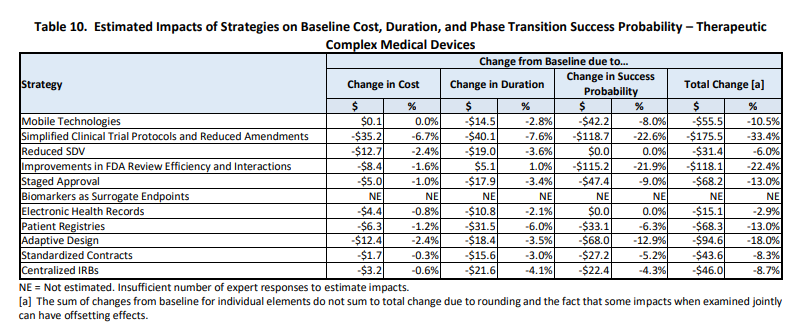
The 2022 ERG study commissioned by HHS shows the strategy with the largest impact on overall development costs is Simplified Clinical Trial Protocols and Reduced Amendments (33.4 percent), followed by Improvements in FDA Review Efficiency and Interactions (22.4 percent) and use of Adaptive Design in clinical study designs (18.0 percent).15
SIGNAL 08. Preventing budget overruns
Only 14% of clinical financial planners at pharma companies are highly confident in their budget forecasts.16
The variance between forecasted and actual clinical trial costs for life science companies can be as high as 16%. Acceptable variance range is 5% to 10%. The top causes of this variance include (a) outsourcing; (b) delays; (c) complexity; and (d) unexpected events. In a blog post last year, WCG wrote:
Across therapeutic areas, we see final budgets today coming in more than 50% higher than at the start of budget negotiation. This outcome begs the question, “Should sponsors start higher?” Is the time spent on negotiation worth the squeeze and the amount of money saved on the back end?”17
SIGNAL 09. Navigating real-world evidence barriers
Real-world data (RWD) is any data that is collected in the context of the routine delivery of care, as opposed to data collected within a clinical trial.
RWD can help to improve the pragmatism and relevance of clinical trials, for example, by adding patient-reported outcomes, by making the intervention more similar to real-life clinical interventions, or by removing unnecessary exclusion criteria. At the Bipartisan Policy Center conference in 2019, then-Commissioner Scott Gottlieb introduced the FDA’s updated RWE policy:
RWD and RWE are already being used extensively for postmarket monitoring of the safety of products during their use in real world settings. To give just a few examples, our use of RWD and RWE, derived from our Sentinel system, eliminated the need for postmarketing studies on nine potential safety issues involving five products, making our post-market evaluation of safety timelier and more effective.”18
Author’s note: The 40-page RWE Program Framework is worth bookmarking if you’re in the drug or biological spaces. For Medical Devices, start with this guidance document.
Setup
Q: How do we optimize clinical trial setup and site management?
SIGNAL 10. Streamlining site selection
Clinical trial site selection can make or break a trial’s success before it even begins, with the average cost to open an investigator site around $50,000.19
And yet, around 11% of sites fail to enroll even one patient.
To start the site selection process, sponsors and/or CROs will send out feasibility questionnaire (FQ) to a list of sites. These are usually printed out and completed by hand. Some questionnaires can take up to 90 minutes to complete and due to the lack of standardization across sponsors and CROs, sites cannot reuse or recycle them.20
After sites complete the FQ, there’s typically a site qualification visit (SQV) to meet site personnel, view the facilities, and review the study protocols and procedures.
Digitizing and standardizing these FQs would go a long way in smoothing the first part of this site selection process. As you might expect, SQVs have changed in the wake of COVID and many are now able to be performed remotely.
SIGNAL 11. Improving site management
Clinical trial site management makes up anywhere from 29% to 59% of the total cost of a trial.
Given that completed clinical trials cost between $44 million and $115 million each, site management represents a significant portion of overall trial spend.21
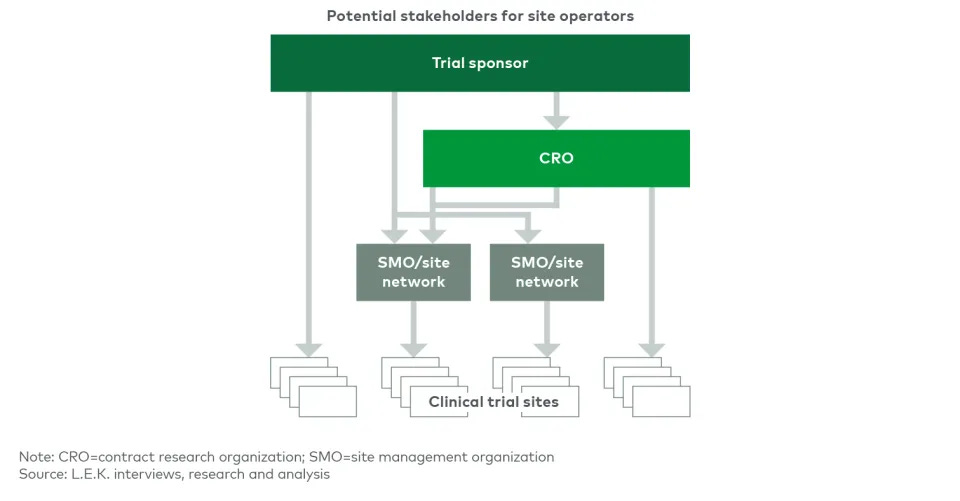
Though site management is less of a focus in the preclinical and earlier stages of trials, end-to-end site management services appear to be going through a bit of a consolidation according to a recent LEK report:
Utilization of Site Management Organizations (SMOs) has been increasing in recent years, especially in complex late-stage trials, and the industry is in the early stages of trial site consolidation under SMO umbrellas, creating more and larger SMO networks.22
Recruitment
Q: What strategies might enhance volunteer recruitment & retention?
SIGNAL 12. Enhancing enrollment and diversity
Only 27% of volunteers screened are eligible to participate in a clinical trial. Current strategies primarily focus on enrolling enough patients to meet endpoints, and they lack proactive targeting to efficiently connect the right patients to the right trials.23
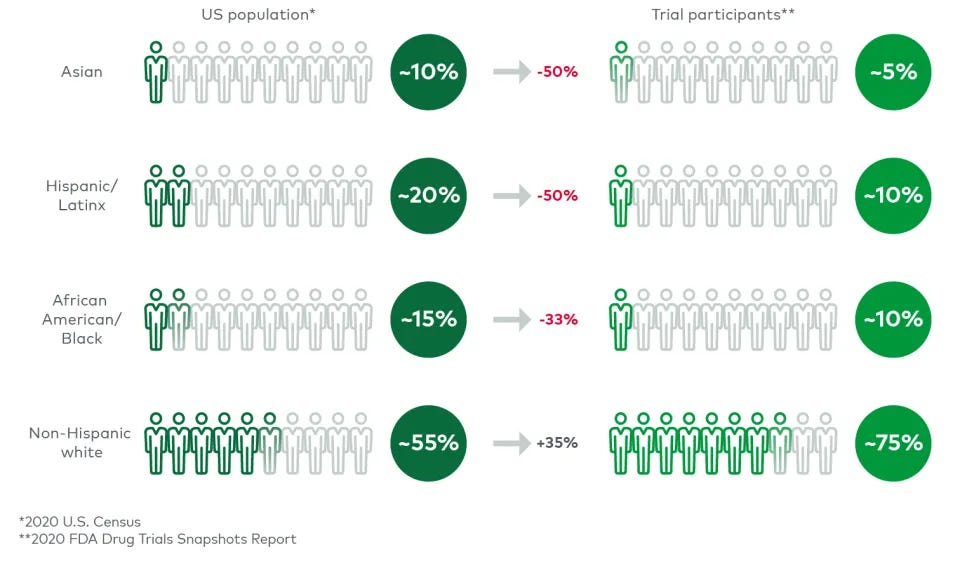
And yet, just 25% of global trial participants are people of color. There is a massive mismatch between enrolled participants and the population, globally and here in the United States.24
Authors of a 2021 Nature paper suggest a socioecological framework to increase diversity in clinical research, which includes changes to public policy, community, institutional, interpersonal and intrapersonal domains.
SIGNAL 13. Boosting participant retention
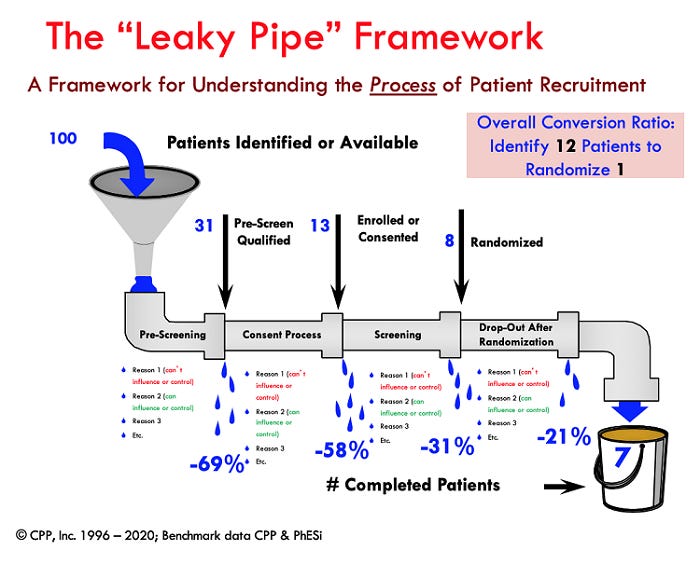
People often describe recruitment as a “leaky pipe” because of how few patients make it through from beginning to end. Out of 100 known patients from the top of the funnel, only 7 will complete a given trial.25
Top reasons people participate include to advance science (43%), to get better treatment for their condition (34%), to receive monetary compensation (34%), for free medication and/or treatment (19%), and because their doctor recommended the study (16%).
Top reasons people drop out include inconvenience, financial constraints, side effects, missed visits, condition not improving, schedule conflicts, misaligned expectations, and even just a change of mind. Importantly, some of these reasons are avoidable.
So what motivates volunteers to continue participation? A 2019 study by CISCRP suggests several steps that can be taken to reduce the number of dropouts along the way:
Minimize burdens during protocol design
Set expectations up-front during informed consent
Explain importance of their participation
Promptly respond to inquiries
Send reminders for upcoming visits
Provide a comfortable and patient-friendly environment
Show appreciation and recognition
Accommodate their schedule as much as possible26
SIGNAL 14. Improving participant compliance
Retention and compliance are closely linked in clinical trials. About 40 percent of patients stop adhering to protocols 150 days into a trial.27
If patients don’t follow rules of the protocol, the data generated during a trial could be incomplete or invalid. About 85 percent of clinical trials wind up being discontinued because they fail to retain enough patients.28
A 2020 Deloitte paper suggests 5 strategies for improving retention and compliance:
Explain expectations early— Patients who understand the expectations of a clinical trial are more likely to comply with the protocols. They also want to know what to expect during each of those visits.
Improve transparency to build trust— Trial sponsors should consider focus groups and trial simulations as they design more patient-friendly protocols. One biopharma company is working to make its clinical trial website patient-friendly and is creating an alumni network so that participants can stay in touch after a trial ends or help inform future trial participants.
Provide real-time feedback— Medication compliance among stroke victims increased by 50 percent when artificial intelligence was used to analyze cell-phone photos to determine whether patients were following protocols.
Tap into behavioral science— We know that one in five prescriptions are never filled, and about half of prescription drugs are taken incorrectly. The use of gamification, nudges, and regular feedback could help encourage better compliance.
Consider remote data collection— Completing tests remotely and transmitting data from home (via connected medical devices) while talking to a doctor via telemedicine could mean patients don’t have to travel to a medical facility as frequently, which could improve their willingness to stay in a trial to completion.29
Conclusion
We made it to the end…of the beginning. Nicely done. In this part of our journey we took a closer look at 14 Signals shaping the preclinical journey, from initial discovery to site selection and recruitment. From speeding up development to enhancing enrollment and retention, the path ahead for bringing safe and effective drugs and devices to market is now a bit clearer. As we delve deeper into this series, we'll begin to weave in case studies, technologies, and key players to help illuminate the potential of clinical research in medicine and our everyday lives.
Part 3: The Trial
In Part 3 of this series, we turn our attention to The Trial, where we delve into site operations, strategies for effective trial management, and real-world case studies from fellow explorers. Join us!
McKinsey, Exhibit 1
Ibid.
NEJM, Adaptive Designs for Clinical Trials, 2016
MDIC, 2016
Nature Reviews Drug Discovery, Phase II and phase III failures: 2013–2015, 2016
JAMA, 2022
HHS, 2022
Applied Clinical Trials, Closing the Variance Gap: The Challenges with Clinical Trial Budget Management and Forecasting, 2015
SAS Global Forum, Optimizing Clinical Research Operations with Business Analytics, 2011
Florence Blog, 5 Strategies for Effective Clinical Trial Site Management, 2023
Nature, Improving diversity in medical research, 2021
CISCRP, Perceptions and Insights Study, 2019
Applied Clinical Trials, Non-Adherence: A Direct Influence on Clinical Trial Duration and Cost, 2017
Clinical Leader, Considerations for Improving Patient Recruitment Into Clinical Trials, 2012
Deloitte Health Forward Blog, Want to improve clinical-trial retention and compliance? Make convenience a priority, 2020