![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!IXc-!,w_120,h_120,c_fill,f_webp,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F9f7142a0-6602-495d-ab65-0e4c98cc67d4_450x450.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!lBsj!,e_trim:10:white/e_trim:10:transparent/h_48,c_limit,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F0e0f61bc-e3f5-4f03-9c6e-5ca5da1fa095_1848x352.png)
Why Kidney Breakthroughs Need Shared Infrastructure
How NURTuRE is linking samples, data, and patient participation for the next era of kidney discovery.

This guest essay is part of our ongoing series highlighting voices across the kidney ecosystem and around the globe. Today’s essay is by Gaia Cantelli, Director of Data Science and NURTuRE at Kidney Research UK.

Kidney data infrastructure is unusually hard to build because kidney disease is not one disease. It is a collection of overlapping conditions that can look similar in clinic but behave very differently biologically. Two people may carry the same broad diagnosis, follow similar care pathways, and still progress for different reasons, at different speeds, and in response to different underlying mechanisms.
That is what makes kidney research so difficult. It is also what makes better research infrastructure so important. The field has never lacked important questions. Why does one person’s kidney disease progress rapidly while another’s remains stable? Why do some treatments work for some people, but not for others? Why are so many people still diagnosed too late, treated too bluntly, or left with options that have changed too little over decades?
Often, the problem is not the quality of the question. It is that the pieces needed to answer it are scattered. A blood sample may sit in one place. Biopsy data in another. Clinical history somewhere else. Patient-reported outcomes may never be connected at all. For researchers, that fragmentation makes important questions harder to answer. For patients, it means progress arrives later than it should.
NURTuRE was created to help solve that problem. Led by Kidney Research UK, NURTuRE is a UK-wide research platform that brings high-quality biological samples together with carefully governed health and research data. Its goal is simple: make it easier for researchers to ask better questions about kidney disease and reach better answers faster.
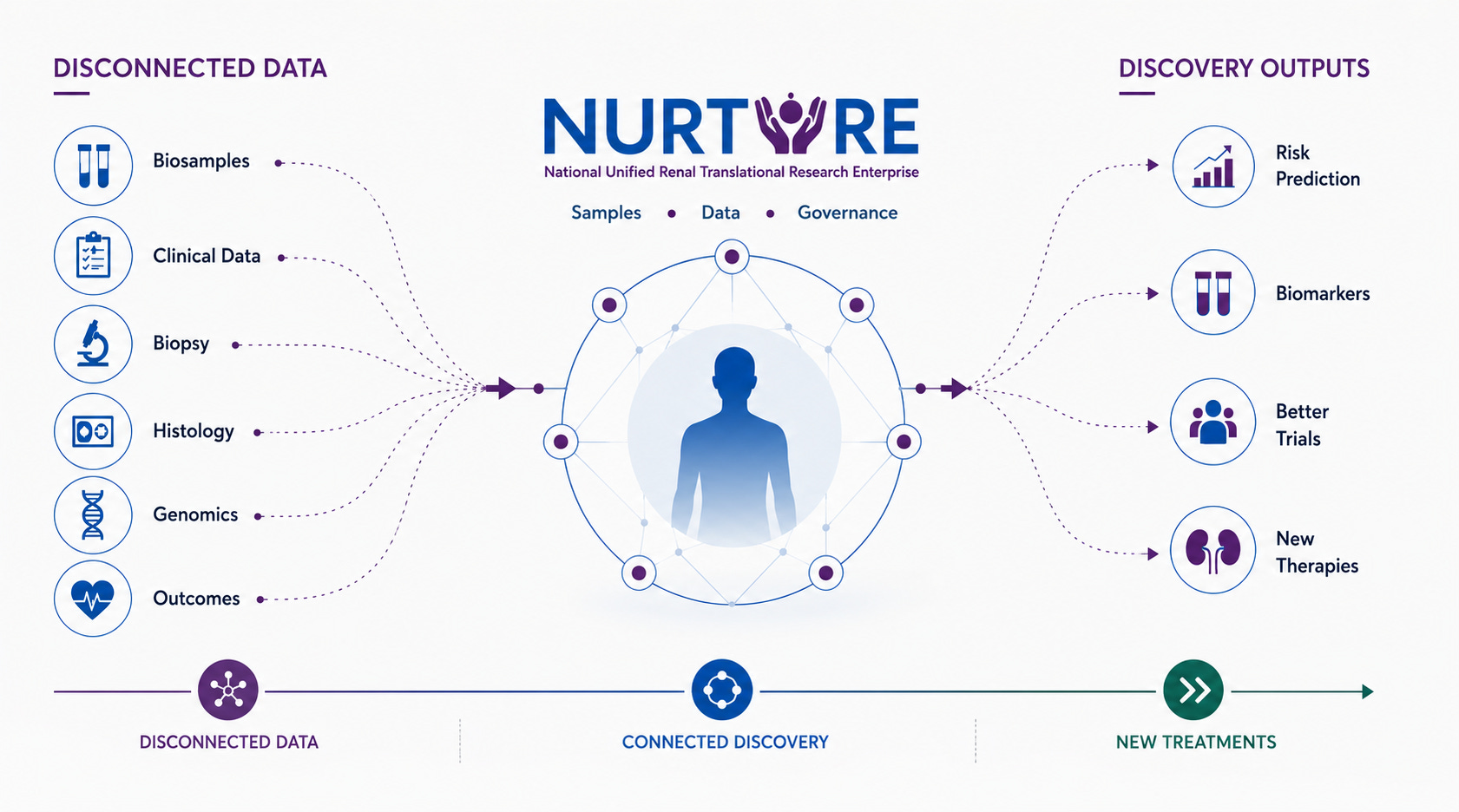
At its foundation are nearly 4,000 people with chronic kidney disease and idiopathic nephrotic syndrome who contributed blood, urine, and detailed clinical information. Their participation created something larger than a collection of samples. It created a platform for discovery, linking serum, plasma, urine, longitudinal clinical data, quality-of-life data, biopsy information, biomarkers, histopathology, whole exome sequencing, and growing multi-omic datasets.
That matters because the most useful kidney data are rarely just numbers in a spreadsheet. A researcher trying to understand why two patients with similar eGFR trajectories have very different outcomes may need more than lab values. They may need tissue, blood, urine, imaging, pathology, genomics, medication history, comorbidities, patient-reported outcomes, and the clinical context that explains how a person’s disease changes over years. Bringing those layers together safely, ethically, and usefully is the work of infrastructure.
Two Cohorts
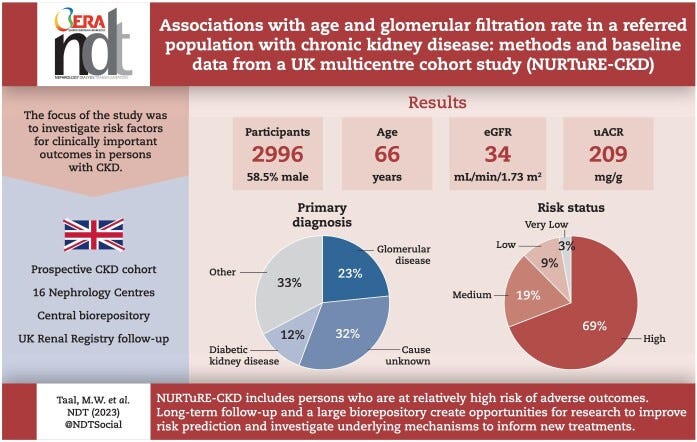
Two NURTuRE cohorts show why this matters. In NURTuRE-CKD, researchers enrolled 2,996 people with CKD from 16 nephrology centers across England, Scotland, and Wales, with clinical outcomes being collected over 15 years through UK Renal Registry linkage. The cohort was built to improve risk prediction and help researchers investigate the underlying mechanisms that drive clinically important outcomes in CKD.1
The NURTuRE-INS cohort adds a different kind of depth. Idiopathic nephrotic syndrome can vary widely from patient to patient, and existing classification systems are increasingly seen as too blunt for the biology underneath. That cohort brings together high-quality biosamples and detailed clinical data from 739 INS patients across the UK, creating a foundation for researchers to study disease mechanisms more directly and develop better ways to subgroup patients.2
Across CKD and INS, NURTuRE shows the promise of shared infrastructure: not just more data, but better ways to understand which patients are at risk, which mechanisms are driving disease, and which treatments may be right for which people.
A Broader Movement
NURTuRE also sits in conversation with major U.S. efforts such as NEPTUNE, the Nephrotic Syndrome Study Network, and the Kidney Precision Medicine Project. NEPTUNE gives researchers access to observational clinical data, histopathology data, biosamples, whole slide images, and derived datasets. KPMP is building a kidney tissue atlas to identify important cells, disease pathways, and potential therapeutic targets in acute and chronic kidney disease.
Taken together, these efforts point toward a different future for nephrology: one built around deeper phenotyping, tissue-based discovery, better biomarkers, and more precise ways to understand disease progression.
NURTuRE brings a complementary UK perspective. It is charity-led, collaborative, embedded in the kidney research community, and designed to connect patient participation, NHS-linked clinical insight, biosamples, and multi-layered data for broad scientific use. That combination feels especially important now.
AI, digital pathology, genomics, biomarkers, and multi-omic discovery are advancing quickly. But these tools are only as useful as the data and biological context behind them. Precision nephrology will not be built on isolated datasets or disconnected samples. It will require shared platforms that allow researchers, clinicians, industry partners, and patients to work from the same foundation.
Success will not be measured only by how many samples are stored or how many datasets exist. It will be measured by whether NURTuRE helps researchers identify earlier signals of risk, understand why scarring develops, improve prediction of progression, support better trial design, enable new partnerships, and move the field closer to more precise prevention and treatment.
The next era of kidney breakthroughs will depend not only on better science, but on better systems for connecting the science we already have.
NURTuRE Biobank is open to all academic and commercial researchers world-wide. To find out more, visit nurturebiobank.org.
Taal MW, Lucas B, Roderick P, et al. Associations with age and glomerular filtration rate in a referred population with chronic kidney disease: methods and baseline data from a UK multicentre cohort study (NURTuRE-CKD). Nephrol Dial Transplant. 2023 Oct 31;38(11):2617-2626. doi: 10.1093/ndt/gfad110. PMID: 37230953; PMCID: PMC10615633.
Colby E, Hayward S, Benavente M, et al. National Unified Renal Translational Research Enterprise: Idiopathic Nephrotic Syndrome (NURTuRE-INS) study. Clin Kidney J. 2024 Mar 30;17(8):sfae096. doi: 10.1093/ckj/sfae096. PMID: 39135942; PMCID: PMC11317841.
 | A guest post by
|