![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!IXc-!,w_120,h_120,c_fill,f_webp,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F9f7142a0-6602-495d-ab65-0e4c98cc67d4_450x450.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!lBsj!,e_trim:10:white/e_trim:10:transparent/h_48,c_limit,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F0e0f61bc-e3f5-4f03-9c6e-5ca5da1fa095_1848x352.png)
Brief: Can Medicare Help More Patients Stay on Home Dialysis?
H.R. 8875 would create targeted payments for in-home support during the most fragile phase of the home dialysis journey. But is it enough?

A home dialysis bill is moving through Congress with a small but important payment signal. Rep. Carol Miller introduced the Improving Home Dialysis Act, which would add two new Medicare-covered support services for patients dialyzing at home beginning January 1, 2028: staff-assisted home dialysis respite care and renal mental health services. The bill applies to support furnished in the patient’s home, excluding skilled nursing facilities and nursing facilities.1
The biggest detail is the budget neutrality waiver. A Ways and Means letter says payment adjustments for both staff-assisted respite care and renal mental health services “shall not be made in a budget neutral manner.”2 Simply put, that means Medicare would not have to fund the new payments by cutting other ESRD payments. If it were budget neutral, the new add-on could simply reshuffle dollars inside the dialysis payment system. With the waiver, it looks more like incremental reimbursement for support that often sits in the gap between what patients need and what the current payment model clearly pays for.
For a sector where small payment changes can shape large-scale protocols and behavior across providers, manufacturers, and care models, that matters. But the bigger story may be less about celebrating a legislative win and more about opening a broader conversation around what meaningful home dialysis support should actually look like in practice.
Background
Home dialysis has long been one of kidney care’s most obvious but under-supported opportunities. Patients often prefer the flexibility and independence of home-based care, but the transition is hard. Training takes time, care partners carry real burden, and early complications can quickly derail confidence. Mental health needs can be significant during this period, yet easy to miss. And for many patients, a temporary illness, injury, or physical limitation can make home treatment feel impossible. That is the practical gap this bill is trying to address: when home becomes too hard for a period of time, the current system does not always give patients or care partners a clear way to get help without risking a return to in-center dialysis.
Two recent reviews help explain why that transition window matters. Home hemodialysis studies report one-year technique failure rates ranging from 2% to 30%, with the highest attrition often occurring early and driven by medical instability, confidence gaps, and patient or caregiver burnout.3 Peritoneal dialysis studies show a similarly wide range, with discontinuation often reported between 6% and 40% depending on the definition and time period, and early failures tied to mechanical issues, peritonitis, psychosocial factors, and late referral.4
I have written about these barriers before. The IM-HOME study helped frame the home dialysis journey as a sequence of barriers across referral, education, training, initiation, and maintenance, with patients, care partners, providers, equipment, home environment, and clinic workflows all shaping whether home dialysis actually works in practice.
Figure: Conceptual model of the patient journey to home dialysis5
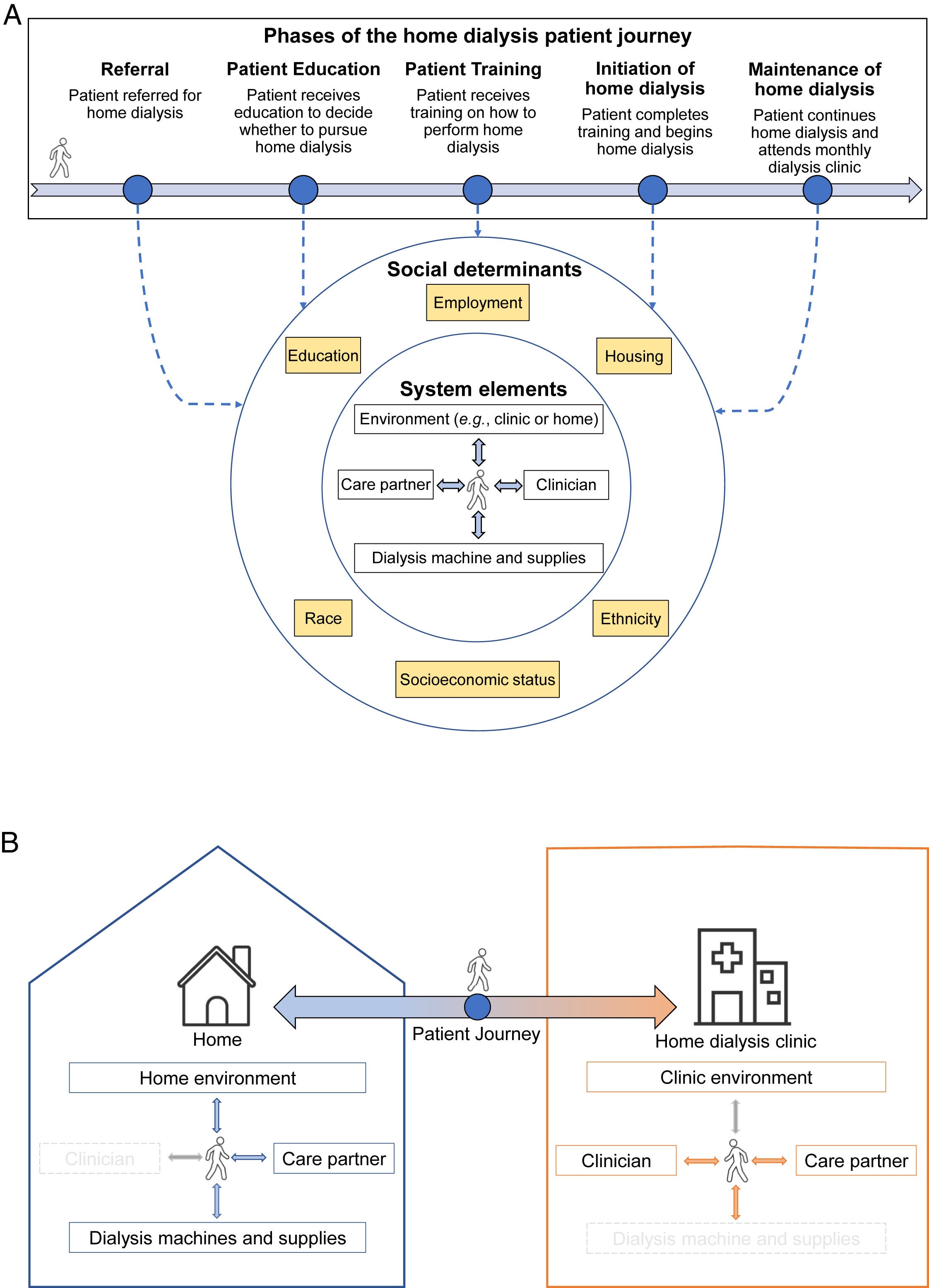
This bill targets that messy middle. Staff-assisted respite care would cover dialysis services furnished by qualified personnel when a home dialysis patient is temporarily unable to dialyze independently. The support would be available during the first 30 days after initiating home dialysis, or at any time if the patient’s limitation is physical. Qualified personnel could include registered nurses, licensed practical nurses, certified patient care technicians, or other qualified medical professionals defined by the Secretary. The bill would also cover up to four renal mental health sessions during the first 60 days after home dialysis initiation.
The National Kidney Foundation called the bill an “important first step” and said it recognizes “the real-world challenges patients and caregivers face while adapting to home-based care.”6
Why it matters
This is not a sweeping home dialysis overhaul. It is narrower, and probably more practical. The bill recognizes that access is not just modality education, equipment, or patient preference. Access also means having enough support to get started, recover from setbacks, and stay home when life gets complicated.
For providers, the proposed payment structure could make it easier to justify staffing models around home starts and rescue support. For patients, it could make home dialysis feel less like an all-or-nothing leap. For the market, it is another sign that policymakers are still looking for ways to move kidney care closer to the home.
Table 1. Illustrative payment impact per home dialysis patient
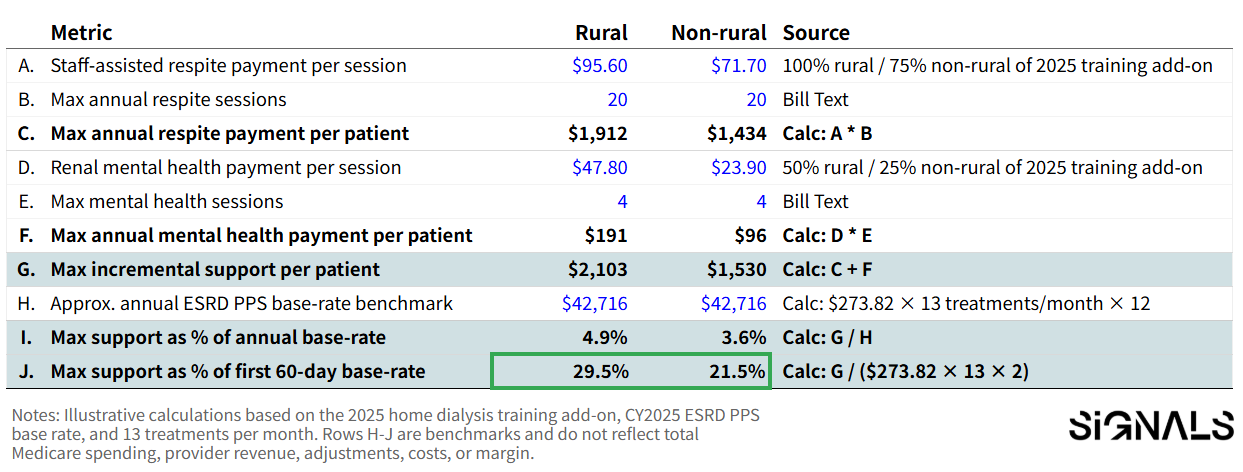
This will not fully solve the economics of assisted home dialysis. Using the 2025 ESRD PPS base rate as a rough benchmark, the maximum support would equal about 3.6% of annual base-rate payments for a non-rural patient and 4.9% for a rural patient. But that may understate the point. These dollars are concentrated around the most fragile part of the home dialysis journey: initiation, early confidence, temporary setbacks, and caregiver strain. Measured against the first two months of base-rate payments, the maximum support could represent roughly 22% to 30% of that early transition window.
At the same time, the payment levels themselves seem low. The non-rural mental health payment in the bill would be roughly $24 per session using the current formula. How should providers realistically deliver meaningful mental health support at that rate?
That is why this matters. The bill does not rewrite the full home dialysis P&L, but it could make the first few weeks at home less fragile and give providers a clearer reason to invest in transitional staffing, rescue support, and mental health resources around home starts.
In my mind, the harder test is whether the bill as written is targeted enough to support the right interventions at the right moments, while still flexible enough to avoid becoming restrictive for the people actually delivering and receiving care in the home.
Timing and market fit
This also lands at a moment when home dialysis is already moving in the right direction thanks to targeted interventions and new payment models. Home dialysis use reached about 15% of new and established ESRD patients in 2023, its highest level in over a decade.
A version of this bill may increase access, but the more interesting test is how much it could change the rate of growth and how existing kidney care models would adapt. As Lekha Tummalapalli and Eugene Lin pointed out in 2022, value-based payment models and capitated Medicare Advantage arrangements would increase interest in home dialysis as a total-cost strategy, while also raising a harder concern: whether some savings depend on costs shifted to patients and care partners through unpaid labor, utilities, and home support.7
Since then, KCC results have shown that value-based kidney models can increase home dialysis, home dialysis training, and optimal ESRD starts, even as the savings picture remains more complicated. That makes H.R. 8875 worth watching as a potential payment layer around the early transition window where home dialysis succeeds or fails. For risk-bearing models, the bigger opportunity may be reducing hospitalizations and adverse events through more frequent home touchpoints. That includes dialysis-related complications like infection, but also broader risks tied to fluid status, blood pressure, medication adherence, and cardiac instability. The bill itself is written around dialysis respite care and renal mental health services, so CMS implementation would determine how much broader monitoring or coordination could be built into the workflow.
The organizations watching this are broader than the usual public-company list. They include large dialysis organizations built around outpatient clinic networks, dedicated home-only providers already building staff-assisted and transitional home models in markets like Chicago, Michigan, Florida, and others, and home care companies that specialize in complex care, social support, and clinical coordination in the home. For each of them, the question is whether this creates a more durable payment layer around the work required to help patients start, stabilize, and remain at home.
That is also why DaVita’s recent investment in Elara felt important. As we wrote in February, the move was less about home dialysis alone and more about building the operating layer for kidney care in the home: staffing, coordination, continuity, and support around complex patients.
The unresolved issue is what kinds of support models policymakers ultimately want to enable. Is the goal narrowly defined respite care, or a broader home support infrastructure that includes in-home training, interdisciplinary support, caregiver relief, monitoring, and flexible workforce models that can realistically scale?
What happens now?
The bill still needs broader support to move, including Democratic support. That is the next real hurdle, especially now. Home dialysis has often been one of the few areas in kidney policy where patient choice, cost management, and care delivery innovation can appeal across party lines.
It also fits into a longer policy arc. The 2019 Advancing American Kidney Health Initiative set a national goal to increase home dialysis and transplantation, and NKF noted that this bill builds on that foundation.8 In that sense, H.R. 8875 is less a new direction than a continuation of an existing federal push to expand treatment options for people with kidney failure.
The policy details will matter. CMS would need to define operational rules, personnel requirements, training standards, billing mechanics, and how these services fit into the ESRD payment system. Those details will determine whether this becomes a meaningful support layer for home dialysis programs or a narrow add-on that is difficult to operationalize and potentially limiting for the providers and patients it is meant to support.
For now, the signal is worth watching. The field has spent years talking about increasing home dialysis, but the support model has lagged the ambition. This bill starts to put payment behind practical services that could make home dialysis more sustainable: help during the first few weeks, support when a patient hits a setback, and mental health resources during a high-friction transition.
What the field is watching
The early response from the field has been encouraging, though many people see this as a starting point rather than a real solution. What types of support actually help patients remain at home? Which workforce models are realistic? What services need to happen in the clinic versus the home? And how should payment be structured so programs can sustainably provide those services without narrowing access?
A new CJASN perspective from Drs. Yuvaram Reddy, Suzanne Watnick, and Nupur Gupta makes a similar point. The authors argue that assisted home dialysis could help more patients, including frail or socially disadvantaged patients, access home dialysis, while noting that current Medicare policy lacks a clear reimbursement pathway for in-home dialysis assistance. They also caution that a nurse-only model would be difficult to scale, which makes the bill’s “qualified personnel” language important. The current text includes registered nurses, licensed practical nurses, certified patient care technicians, and other qualified medical professionals specified by the Secretary.
That may be the most important takeaway from this version of the bill. The field still needs clearer input from the people closest to this work: patients, care partners, social workers, home dialysis educators, nurses, technicians, and providers actively delivering care in the home. If policymakers want these models to succeed in the real world, they need to understand what support is actually feasible, useful, and sustainable at the bedside and in the home.
I’d love to hear what you think: can targeted payment support make home dialysis more accessible, and what would need to change for this type of policy to be truly workable in the real world?
Author’s note: My thanks to everyone who shared thoughts and experiences that helped shape this piece, especially patients and care partners who know these hurdles firsthand and the many clinicians, operators, and advocates working to help more people realize the benefits of doing dialysis at home.
H.R.8875 - Improving Home Dialysis Act:
https://www.congress.gov/bill/119th-congress/house-bill/8875/
Ways & Means Views & Estimates Letter:
https://waysandmeans.house.gov/wp-content/uploads/2026/05/H.R.-8875-AINS.pdf
Tran, E., Karadjian, O., Chan, C.T. et al. Home hemodialysis technique survival: insights and challenges. BMC Nephrol 24, 205 (2023). https://doi.org/10.1186/s12882-023-03264-5
Paola Piarulli, Valerio Vizzardi, Federico Alberici, Hilary Riva, Marta Aramini, Luca Regusci, Pietro Cippà, Antonio Bellasi, Peritoneal dialysis discontinuation: to the root of the problem, Journal of Nephrology, Volume 36, Issue 7, 1 September 2023, Pages 1763–1776, https://doi.org/10.1007/s40620-023-01759-w
Reddy Y, Kearney M, Ward M. Identifying Major Barriers to Home Dialysis (The IM-HOME Study): Findings From a National Survey of Patients, Care Partners, and Providers. American Journal of Kidney Diseases, 2024; 84, 567-581.e1
Home Dialysis Bill Signals Progress In Treatment Access:
https://www.kidney.org/press-room/home-dialysis-bill-signals-progress-treatment-access
Tummalapalli SL, Lin E. Is Home Dialysis the Way Forward for Medicare? Assessing Potential Cost Savings Associated with Peritoneal Dialysis. J Am Soc Nephrol. 2022 Nov 1;33(11):1963-1965. doi:10.1681/ASN.2022091017.
Advancing American Kidney Health:
https://aspe.hhs.gov/sites/default/files/private/aspe-files/262056/advancingamericankidneyhealth.pdf
As a longtime believer in home dialysis, I think this is a very positive step. One of the biggest challenges providers face is not getting patients to choose home therapy, but helping them successfully navigate the first 90 days, when confidence is still developing and dropout risk is often highest. The additional support for respite care and mental health recognizes the reality that patients and care partners need more than training and equipment to succeed at home.
While this bill alone will not solve all the barriers to home dialysis, it creates an important step that support services have value and may deserve dedicated reimbursement. Anything that helps providers invest in transitional support, patient confidence, and retention has the potential to improve long-term outcomes and help more patients remain successfully at home.
That said, even if the legislation passes, there is still significant work ahead to operationalize these services effectively. Funding alone will not solve the challenge. Success will require thoughtful collaboration among providers, care teams, technology partners, and manufacturers to determine how support is delivered, who provides it, how patients are identified for intervention, and how outcomes are measured. The opportunity is not simply to add services, but to build a sustainable support ecosystem that helps patients thrive at home long term.