![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!IXc-!,w_120,h_120,c_fill,f_webp,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F9f7142a0-6602-495d-ab65-0e4c98cc67d4_450x450.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!lBsj!,e_trim:10:white/e_trim:10:transparent/h_48,c_limit,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F0e0f61bc-e3f5-4f03-9c6e-5ca5da1fa095_1848x352.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!NnOt!,w_144,h_144,c_fill,f_auto,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F688fc47b-7202-4a2e-b4f4-fea2b047ab1b_1500x1500.png)

Alport syndrome has long been underdiagnosed, misunderstood, and without an FDA-approved treatment. But that may be starting to change.
In this conversation, Lisa Bonebrake, Executive Director of Alport Syndrome Foundation, shares how her own family’s diagnostic journey led her into patient advocacy, and how ASF is now helping bring patients, clinicians, researchers, regulators, and industry to the same table. We discuss the rise of genetic testing, the growing Alport therapeutic pipeline, the role of patient registries and real-world data, and ASSENT, a global effort to support clearer surrogate endpoints and a more predictable regulatory pathway.
Nearly a century after Cecil Alport first described the condition, this rare kidney disease community may finally be entering a new chapter: clearer diagnosis, better data, and a path toward approved treatments. Thanks for being here with us.
About Alport Syndrome
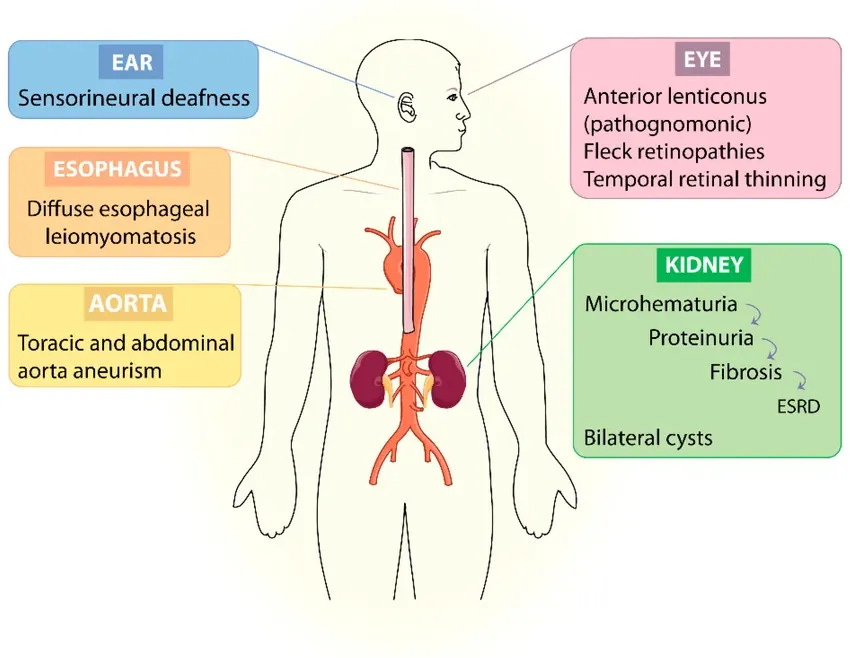
Alport syndrome is a rare genetic kidney disease that can affect the kidneys, hearing, and vision. For many families, the journey to diagnosis can take years, which is why genetic testing, patient education, and advocacy have become so important. Alport Syndrome Foundation is the leading patient-led nonprofit supporting the Alport community. Learn more here.

Q&A
Let’s start with you. Tell us about yourself and the work you do at Alport Syndrome Foundation.
Lisa: I’m grateful for the opportunity to highlight the work we do because this is not only a career for me, it’s also personal. I am an Alport syndrome patient, the parent of a patient, and the parent of a living donor.
At Alport Syndrome Foundation, our work is to provide education and support, collectively invest in research, and support industry in the mission to find potential treatments for Alport syndrome. That is the goal.
We have more than 11,000 members, primarily in the United States, but about 14% are outside the U.S. There are many countries that do not have a patient organization, so people often turn to us. That means using Google Translate and other tools, whatever it takes, to help patients gain an understanding of what it means to live with Alport syndrome.
Can you share more about your family’s story?
Lisa: My story is really not uncommon in our community. I hear it reflected back to me often when I meet other patients and families across the U.S. and around the world.
I grew up living with kidney disease and was misdiagnosed for more than 40 years. I had children not knowing I had a genetic kidney disease that I could pass down. My oldest son did not receive my genetic mutation, but my youngest son did, and he started having symptoms very early.
At the time, I was told, “He has what you have, and he’ll be just fine.” So we missed out on some years of treatment and monitoring. Then, when he developed hearing loss, which can also be caused by Alport syndrome, I was told it might be cancer, a brain tumor, or many other things.
Eventually, I went online and searched “boy,” “kidney disease,” and “hearing loss.” Articles about Alport syndrome came up. When I read through them, they really resonated with me. I thought, this must be the underlying cause of the kidney disease in my family.
It took a while to get someone to listen, but I finally found a nephrologist who was trained in both pediatric and adult nephrology, which is rare. We call her a “unicorn.” She took us seriously and was able to get us a biopsy right away. That was how Alport syndrome was first confirmed in our family.
Then we found Alport Syndrome Foundation. They treated us like family. They connected us to educational resources, experts in the disease, and research for the first time. That changed everything for my family.
I became involved as a volunteer, then joined the board, and later became staff. This work is deeply important to me, both personally and professionally.
What has changed the most since you first started learning about Alport syndrome?
Lisa: There have been some really big changes.
The first is genetic testing. Genetic testing has changed the game in Alport syndrome. When I first started this work, it was very rare for someone to join our free membership and report that they had a confirmed genetic diagnosis through genetic testing. Most people had been diagnosed by biopsy or were suspected to have Alport syndrome based on family history.
Now, more than 90% of our members who come on board each year self-report that they have had genetic testing and understand their genetic type. That is a tremendous sea change for research and for attracting companies into our space to think about treatments.
It has also shown us just how underdiagnosed Alport syndrome has been for so long. So many patients had stories of misdiagnosis. We were a community that was misunderstood and underdiagnosed. Genetic testing has changed that. The work Natera has done, with more than 14,000 individuals identified with genetic test results consistent with Alport syndrome, tells an important part of that story. People are being diagnosed more accurately and earlier, which also opens the door to potential earlier treatment.
The second major change is the therapeutic pipeline. When I started this work, there was one company with an Alport program and one clinical trial that started shortly after I began working with ASF. That drug was not approved, but at the time, it was one company.
Now there are six active clinical trials in our space that are either directly for Alport syndrome or include an Alport cohort within a basket study. There are also more therapies advancing toward the clinic quickly.
And the third big change is genetic therapies. Genetic therapies are moving toward the clinic very quickly. That is tremendously exciting and brand new for us.
What role does a patient organization play in helping companies develop new therapies?
Lisa: I don’t think the role of patient organizations on the front end of drug development is always clearly understood in the kidney ecosystem yet. But organizations like Alport Syndrome Foundation can be powerful conveners.
We are credible messengers of the patient voice. We have a contact database. We know where patients live. We understand where genetic testing is happening. We can get messages to patients so they are educated about their disease and about opportunities to participate in research.
We run our own patient registry. We have collectively invested as a community in a natural history study in partnership with NEPTUNE, a research consortium in the kidney space. That allows us to help bring patient data and the patient voice into the research process.
Just as importantly, we help make sure patients are protected, their privacy is respected, and their perspectives are heard in drug development. As a convener, we work with regulators, genetic counselors, researchers, clinicians, industry, and patients.
That role matters. We can help companies understand the patient experience quickly. For example, we offer patient listening sessions at no cost. A company can come to us and say, “We’re developing this protocol. How will patients see it? Will this work for them? Do they have concerns? Does it fit their lifestyle?”
We can bring patients together in person or virtually, and pharma has told us those sessions are tremendously helpful. The goal is to help companies invest wisely in Alport syndrome and use their dollars and intellectual resources well.
It sounds like a win for both sides. Who else needs to be at the table?
Lisa: There are a lot of people we need at the table. We need industry. We need genetic testing. We need qualified genetic counselors who can help patients understand their genetic test results, what those results mean for their own kidney disease risk, and who else in their family may be at risk.
We need regulators, and I’m grateful to say the FDA has been working with us as a partner in this space.1
We need everybody at the table.
How significant is genetic testing to where Alport syndrome goes from here?
Lisa: It is incredibly significant. Patients come to genetic testing in different ways. Some have a suspected diagnosis and come to us directly asking, “How do I get genetic testing?” We provide options and information about their right to testing, what they might learn, how it could shape their treatment plan, and what it could mean for their family.
We are also seeing more people learn about Alport syndrome during family planning. They may use a test like Natera’s Horizon program to understand what risks may exist in their family. So we are seeing more people come to us very early, even before they have children.2
Others come through nephrology. They may have hematuria or proteinuria and not know why. A clinician who understands the role of genetic testing may order a test, and that is becoming more common. Genetic testing is now part of the KDIGO guidelines for patients with certain symptoms, which is an important change.
In our experience, pediatric nephrologists embraced genetic testing a little faster than adult nephrologists, although that is beginning to change. They have really been on the front lines.
We also hope more clinicians will refer patients to Alport Syndrome Foundation when they are diagnosed, because people need support, education, and community. Everything ASF does is free.
How does ASF support patients across the diagnostic and care journey?
Lisa: We have information to help people understand their right to genetic testing. We also backchannel with some companies if patients are struggling to pay for testing, because it is so important for families to understand their diagnosis, get the right treatment, and understand their risks.
We also have a large support community. For example, we have an online support group that is only open to patients and caregivers. It has more than 6,100 people and is moderated by ASF staff and volunteers 24/7.
People are exchanging real experiences in real time and helping each other through this. I find it tremendously valuable. It has helped my own family, and I see it help so many others.
You mentioned registries and longitudinal data. What does that work look like, and why does it matter?
Lisa: These days, data is everything, particularly in a rare disease that is not well understood. Alport syndrome has different genetic types: autosomal recessive, autosomal dominant, X-linked, and digenic. It is also a complex disease. It affects the kidneys, but it can also affect the ears, eyes, lungs, and heart. So we need data to understand the wide variety of patient experiences, the risk of kidney failure across genetic types and variants, and the other symptoms that come with the disease.3
ASF also sponsors its own registry, which was established in 2023. It includes self-reported data, but patients can also upload genetic test results, audiograms, lab reports, family history, medications, doses, and information about side effects. Genetic test results are verified by medical genetics specialists on the back end, so researchers and pharma can trust that data.
That will become especially important if new treatments are approved, because we will be able to understand how patients are using them in the real world.
One of the biggest challenges is that registries are often siloed, and it is difficult to share data. This is where a patient organization can come in and cross borders in ways that others may not be able to.
We are working with registries around the world to collect, harmonize, and analyze data in a public-private partnership with the FDA. The goal is to inform the use of surrogate endpoints in Alport syndrome. We are starting with eGFR and proteinuria, so those measures are better understood and could potentially support a clearer regulatory pathway. With a rare disease, there is not one country or one database with enough data in one place. You need global collaboration. That is where we can help convene.
How common is Alport syndrome?
Lisa: I wish I could give a definitive answer, but prevalence is still a bit of a mystery. The studies have limitations, and the estimates have changed over time.
What we are finding through increased genetic testing in the U.S. and places like the U.K. is that Alport syndrome is far more common than we ever would have imagined. We are proving that, even if we do not yet know the exact prevalence.
A few years ago, Dr. Alexander Chang and colleagues conducted a study at Geisinger Health. Dr. Chang is now co-chair of the international data collection project we are working on called ASSENT. His study found that X-linked Alport syndrome had a prevalence of about 1 in every 2,000 individuals in that health system.
What we are also finding is that autosomal dominant Alport syndrome is far more common than that. Some studies suggest autosomal dominant Alport genetics may be present in as many as 1 in 100 births. But the experience is highly variable. Some people may never have symptoms, never be tested, and never experience kidney disease progression.
What we need to understand is why some people with autosomal dominant Alport syndrome have the full Alport experience and progress to kidney failure. Is it the variant? Is it environmental factors? We do not know yet. That is another reason why collecting this data is so important.
Can you tell us more about ASSENT and the work to build a clearer regulatory pathway?
Lisa: ASSENT stands for Alport Syndrome Surrogate Endpoint Network. It came out of a research and regulatory workshop that Alport Syndrome Foundation convened in May 2025. We brought together members of the FDA, representatives from NIH, and about 30 of the world’s leading experts in Alport syndrome, including researchers and clinicians who see and treat many Alport patients.
The question was: how do we build a clearer regulatory pathway for a growing pipeline of potential treatments in Alport syndrome?

What we realized is that the human data had not yet been analyzed in a way that could inform surrogate endpoints. We need to better understand the biomarkers that predict risk of kidney failure in Alport syndrome. You do not want trials that have to last for years and years, waiting for people to progress to kidney failure. You want to understand risk earlier.
That is where ASSENT came from. Someone needed to collect and analyze the data, and ASF was encouraged to be the convener because we had already shown we could bring global experts and regulators together.
The work is being done by extraordinary volunteers: biostatisticians, renal endpoint experts, clinicians, and researchers. We now have a data coordinating center, and registries and dataset holders from around the world have signed on to participate.
What has been powerful is hearing clinicians say they are volunteering because they are tired of having no approved treatments for their Alport patients, many of whom progress to kidney failure early in life. This gives them a meaningful way to help shape a new path toward potential treatments.
What is the timeline for ASSENT?
Lisa: We had our first meeting with FDA liaisons in December 2025 to share the statistical analysis plan. They graciously gave us a five-hour in-person meeting on the FDA campus, and we came away with agreement that the roadmap made sense. Since then, we have been identifying data sources, getting participants on board, and refining the statistical analysis plan.
Our next in-person meeting with the volunteers, committee members, and FDA liaisons is in June 2026 in Washington, DC. The goal is to review the initial analysis from several registries, work through remaining questions, and finalize the statistical analysis plan.
Then, at the International Workshop on Alport Syndrome in Budapest on September 5, we will hold a workshop focused solely on ASSENT. We will share the first set of analyses and give everyone a chance to ask questions, provide feedback, and think through the findings. The hope is to complete the analysis early next year. We have to follow the science. We do not know exactly where it will lead, but we hope it will bring real clarity.
How can patients participate in this effort?
Lisa: Patients around the world are participating by contributing their data to patient registries, including the ASF Alport Patient Registry here in the U.S.
We try to keep patients informed through our monthly e-newsletter, which goes out to free members, clinicians, researchers, and industry members. We also share updates through social media and on our website, where we have information and a video about the project. Right now, the main way patients are involved is by contributing their data through registries.
What are your top priorities for ASF over the next year or two?
Lisa: Next year is a big milestone year for us. In 2027, it will be 100 years since Cecil Alport published his paper describing families with kidney failure early in life and hearing loss. It will also be 20 years since Alport Syndrome Foundation was established.
So it is a chance to look back at the progress we have made, but also to look ahead. One major priority is completing this international data collection project, which we hope will inform the use of surrogate endpoints and help open a clearer regulatory pathway for Alport syndrome. We will be doing a lot of celebrating next year, but what I really hope is that 2027 and 2028 bring the first approved treatments for Alport syndrome. That would be fantastic.
Another major priority is preparing for genetic therapies. These are advancing quickly, and there is a lot of work to do. For example, we need to better understand the role of biopsies in adults and pediatrics, and what they may contribute to understanding treatment effect.
Not long ago, we thought genetic therapy might be science fiction for Alport syndrome. That is no longer the case.
Final thoughts? What do you want people to take away from this conversation?
Lisa: I want everybody in the nephrology space to understand the role patient organizations like Alport Syndrome Foundation are playing on the front end of drug development.
We can bring real value as a partner. We are part of the data ecosystem. We help patients understand their right to participate in research. We connect companies with clinicians, trial sites, and thought leaders. We provide real-time patient feedback on protocols. And we help make sure companies are investing wisely in Alport syndrome.
This work is also about patient empowerment. Patients want to be involved. We know we can bring value through our lived experience. We are experts in our disease in a different way, and those insights matter.
So I would say to anyone in nephrology, whether you are a researcher, clinician, genetic counselor, policymaker, or industry leader: come to us early. Most of our research funds come from patients, families, caregivers, and friends who love them. This is an important role we have to play, and we take it seriously.
###
We’d love to hear from you. What stood out from Lisa’s story, and what should more people understand about Alport syndrome, genetic testing, and the role patients and families can play in advancing care?
Learn more about the ASF-FDA meeting that took place on December 5, 2025 at the FDA White Oak Campus in Silver Spring, Maryland here.
Souter, V., Johnson, L., Becraft, E., Cantu-Weinstein, A., Tabriziani, H., Benn, P., & Kashtan, C. E. (2025). Carrier screening for Alport syndrome: The clinical importance of heterozygosity for pathogenic or likely pathogenetic variants. Journal of Genetic Counseling, 34, 1–6. https://doi.org/10.1002/jgc4.70045
Martínez-Pulleiro R, García-Murias M, Fidalgo-Díaz M, García-González MÁ. Molecular Basis, Diagnostic Challenges and Therapeutic Approaches of Alport Syndrome: A Primer for Clinicians. International Journal of Molecular Sciences. 2021; 22(20):11063. https://doi.org/10.3390/ijms222011063
