![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!IXc-!,w_120,h_120,c_fill,f_webp,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F9f7142a0-6602-495d-ab65-0e4c98cc67d4_450x450.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!lBsj!,e_trim:10:white/e_trim:10:transparent/h_48,c_limit,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F0e0f61bc-e3f5-4f03-9c6e-5ca5da1fa095_1848x352.png)

Kidney transplant is one of medicine’s great success stories. For many patients, it offers years of life, freedom from dialysis, and the chance to return to school, work, family, and plans they may not have thought possible.
But the work does not end after surgery. After transplant, patients and care teams enter a long period of surveillance. Labs, clinic visits, medication changes, infection monitoring, antibody testing, and sometimes biopsies all become part of the rhythm of life with a transplanted kidney. The goal is simple, but difficult: catch problems early enough to protect the graft.
One of the hardest problems we have yet to solve is antibody-mediated rejection, or AMR. AMR occurs when the recipient’s immune system attacks the transplanted kidney, often involving donor-specific antibodies and inflammation in the kidney’s small blood vessels. It has emerged as a leading cause of late kidney allograft loss, and treatment has historically been limited, heterogeneous, and difficult to standardize.1
That reality sits at the center of this conversation. The future of transplant is not only about getting more people transplanted, it is also about helping every donated kidney last as long as possible.
Participants
Matthew Cooper, abdominal transplant surgeon, Chief of Transplantation and Director of the Solid Organ Transplant Line at the Medical College of Wisconsin
Mary Baliker, four-time kidney transplant recipient, public health professional, and longtime advocate for patient-centered transplant care
Uptal Patel, adult and pediatric nephrologist, former transplant nephrologist at Duke, and head of Biogen’s West Coast Hub focused on kidney disease and transplant innovation
What’s inside
How post-transplant monitoring works today
Why kidney rejection can be difficult to detect before damage occurs
What AMR is and why it matters for long-term graft survival
How patients experience the lifelong burden of vigilance
The role of biomarkers, biopsies, and donor-derived cell-free DNA
Why new therapeutic innovation may change the urgency of early detection
Biogen’s role in advancing felzartamab to Phase 3 trials for late AMR
What a more proactive post-transplant model of care could look like
Q&A
How does post-transplant monitoring work today?
Matt: There are standards that all transplant programs follow, but there are also nuances based on training, experience, and the complexity of the patient. Follow-up is much more concentrated early after surgery, then becomes less frequent as patients move further out from transplant. But the desire is always to be proactive rather than reactive.
We are all fond of the kidney because it does so many amazing things, but it often does not give us clinical symptoms when something is wrong. We tell patients, “Let us do the busy work of assuring that everything that feels good and natural continues to look good when we do labs and other investigations.” In our clinic, patients usually come back twice a week for the first couple of weeks. They have blood work drawn, urine samples checked, and we look at markers of kidney health. We also monitor for signs of over-immunosuppression, including BK virus and cytomegalovirus, or CMV.2
We also think about the patient’s risk for rejection, whether cellular rejection or antibody-mediated rejection, and we check donor-specific antibodies at particular time points based on our protocol. Donor-specific antibodies, or DSAs, are antibodies that a recipient may develop against the donor organ and are an important risk factor for AMR and graft loss.3
All of this happens with surgeons, nephrologists, coordinators, and the rest of the transplant team. It is spelled out in the medical record and in the documentation we give patients when they leave the hospital because we want them to understand why we are doing all of these things. We also want them to know this has to be a partnership going forward.
Mary, what was monitoring like from your side?
Mary: My post-transplant monitoring was very rigorous. There was intense surveillance at the beginning, and then it moved into long-term maintenance. At home, I tracked my temperature to check for signs of infection. I checked my blood pressure to watch for medication side effects. I tracked my weight to see if I was retaining fluid.
Then there was the lab work. Early on, I was having labs drawn multiple times a month. Over time, that shifted to monthly. Clinic visits were frequent at first too. I always describe it as having all eyes on me, making sure everything was together. And it really was multidisciplinary. I had the transplant surgeon, transplant nephrologist, pharmacist, transplant coordinator, and dietitian. That monitoring was such an important part of care.
Why is there so much variability across transplant centers?
Uptal: First off, transplant care is incredibly complex. The medical and surgical management is complex, and the tools available to us have been evolving. But there is also incredible variability because we do not always have high-grade evidence for best practices. We have options. We have clinicians who trained in different programs and learned different ways of doing things. Outcomes are not always dramatically different, so people can get stuck doing things the way they have been done around them.
That variability shows up at the system level too. Despite efforts to standardize care through quality oversight, data remain fragmented across health systems. Patients receive care in different parts of the healthcare system, and every transplant center has to deal with that. It also shows up in biomarker use. When we look across centers and try to identify patients, including for clinical trials, we see tremendous variation in which biomarkers are used and how frequently they are used. Variation by itself is not always a problem. But if we are not identifying patients who are developing complications from transplantation, then it is worth reexamining how we can organize ourselves better.
Why is rejection so hard to detect early?
Matt: The immune system is something we continue to learn about all the time. Every time we think we have figured it out, we realize each person responds a little differently to a kidney transplant. The immune system continues to evolve and adapt. As providers, if we are trying to be proactive rather than reactive, we are constantly looking for tools that help us get further upstream in the pathology of rejection.
We have valuable tools now, including biomarkers. But traditional tools like serum creatinine and urine protein are nonspecific and not very sensitive. By the time we see changes, we may already be behind the eight ball. We used to biopsy patients all the time. We had a biopsy protocol where every patient, depending on risk, might receive a biopsy at one month, three months, and one year. As a surgeon, I always say that if you have not seen complications from biopsies, you have not done enough of them.
So we began using tools like cell-free DNA, gene expression profiling, and molecular microscope approaches. We moved away from protocol biopsies as the only standard and started using technology to be better purveyors of biopsies. We biopsy less, but with better indications. That said, we still need better technology and better tools to identify rejection earlier.
Uptal: The deeper breakdown is the failure to identify immune attacks before irreversible organ damage has occurred. The delay happens because standard monitoring usually falls back on kidney function. But kidney function lags behind the immune injury. There is a period between the time there is enough immune signal to warrant action and the time visible damage has occurred.
That is where evolving tools may help us make more informed decisions about how and when to use biopsies. Biopsy has been the gold standard for a long time, and it remains important. But complications are real. Donor-derived cell-free DNA, or dd-cfDNA, is one example of a noninvasive blood-based biomarker that can signal injury from the transplanted organ, although it does not tell you the cause of that injury by itself.4 Then, once we get into tissue, newer tools like gene expression profiling can complement what we see under the microscope and give us a more refined understanding of immune activity.
Mary, what is it like to live with that uncertainty?
Mary: As a transplant recipient, I feel like I live in this dual state of reality. There is deep gratitude for the gift of life and the second chance at life. But it is paired with a chronic fear that the gift could disappear at any time, at any moment. I know that better than most, having had four kidney transplants. You never lose that fear. I am 27 years out with my fourth transplant, and I know there is still a chance something could happen.
When did you become an activated patient?
Mary: My story may be a little different because I was diagnosed with kidney disease when I was nine years old, and I had my first transplant as a teenager. I became an activated patient with my first transplant. Part of that was because my transplant surgeon said to me, “You know your body better than anyone else.”
That was life-changing. It validated me. It shifted me from being a passive recipient of medical care to being the captain of my healthcare. My early training was learning the visual appearance of my pills, memorizing the signs of rejection, and really owning my care. I think that should be the gold standard for patients.
What should patients ask their care team?
Mary: Patients should see themselves as part of the team. Shared decision-making is important. What are your goals? What do you want from this transplant? What kind of life are you trying to get back to? For me, transplant gave me the opportunity to go to college, which I never thought I would see because I honestly did not think I would live long enough.
Patients should also ask about monitoring. Other than biopsy, what else can we do that is less invasive? What is happening in the field? What tools are available? If you have questions, go to your providers and talk to them. You should feel educated on what you need to know to have the best quality of life possible.
How do you think about shared decision-making?
Matt: The important point is that asking questions is a good thing. I never fear when someone asks questions because it tells me they recognize both the responsibility and the partnership we are engaging in. We try to create that partnership well before surgery. We often have months before a transplant, especially with living donor transplants, so we work to build collaboration ahead of time.
I love what Mary said because we ask the same kind of question: What does transplant mean to you? What are you looking forward to after transplant? Everyone has a different answer. Everyone’s story is a little different. But we want to help them meet that expectation. At the same time, we are not with patients 24/7. We need them to take medications, come to appointments, and get labs drawn. The challenge is that the further people get from transplant, the less frequently we see them. If patients are the captains of their health and are comfortable connecting with us when something is out of the ordinary, the relationship becomes much more seamless.
What would a more proactive model look like?
Uptal: We started with variability, and that variability exists at the system level, provider level, and patient level. Part of moving forward is recognizing the value of early detection. Another part is the availability of new treatments, because new treatments increase attention to early detection.
We have seen that in IgA nephropathy, a relatively common glomerular disease. As disease-modifying treatments become available, practice patterns change. Clinicians act on tests differently. They test more thoroughly. They recognize the disease earlier. Something similar could happen in transplantation if the treatment landscape evolves.
At the system level, centers need access to the right tools, whether locally or externally. At the provider level, there needs to be awareness and comfort with those tools. Then, at the patient level, monitoring should be personalized. Several years after transplantation, one patient may want a different level of noninvasive monitoring than another patient. The point is to use the tools we have to create more informed discussions with patients.
Where do you see the field moving?
Matt: One challenge in becoming more proactive is that even if we identify AMR, we have not historically had great tools to treat it. In some respects, I think the field became a little apathetic. Maybe that is not the best word, but it is real. Over the course of my 25 years, we investigated a number of interventions that did not achieve our goals.
Now it is incredibly exciting to see what is coming. I just spent several days at the American Transplant Congress, where a lot of this science was coming forward. Some of the opportunities we are seeing have re-engaged our interest in early identification because we may now have something to treat people with.
We also have to recognize that our clinics are already full. A lot of this will need to happen in the outpatient setting. There is enthusiasm around urine-based biomarkers that patients could potentially use at home. That would be exciting. But we still need to explain to patients why ongoing monitoring matters. Why do we still want labs monthly when someone is six, seven, or eight years out? Because we want to stay ahead of this. I do not think we should completely get away from biopsies. Biopsy is still the gold standard. But better biomarkers could help us know when a biopsy makes sense.
Mary, what is your reaction to a more proactive model?
Mary: To me, it is exciting. A proactive model shifts the focus from reactive crisis management, where we fix problems after they happen, to anticipatory and integrated care. It is about preventing clinical and systematic failures before they occur. It also validates the patient experience. Instead of forcing patients to fight the system to be heard, the model honors what patients know about their bodies.
Patient self-tracking, physical intuition, and clinical evidence all matter. What patients are saying is not an annoyance. We are bringing something to the table. I think about my own history with antibody-mediated rejection. What could we have done differently? Was there something we could have caught earlier so I would not have lost my third transplant?
There is also a mental burden. Patients often feel like they have to be the project manager, pharmacist, insurer, and everything else. A more proactive system could take some of that weight off patients and allow us to spend more energy living life, not just keeping the kidney alive.
Why did Biogen invest in transplant?
Uptal: It is an interesting story, and it began before my time. The people who deserve the highest credit are Dr. Georg Böhmig at the Medical University of Vienna and Dr. Klemens Budde at Charité University in Berlin. They had the insight that targeted anti-CD38 therapies could be very effective in treating AMR.5
The dominant paradigm at the time was that donor-specific antibodies were the central driver of this disease process. AMR accounts for much of the late allograft loss we see in transplantation. Acute rejection rates have improved dramatically over the past 30 to 40 years, but we have not made a real dent in long-term graft survival. That is likely related to chronic allograft rejection, much of which we recognize as antibody-mediated.
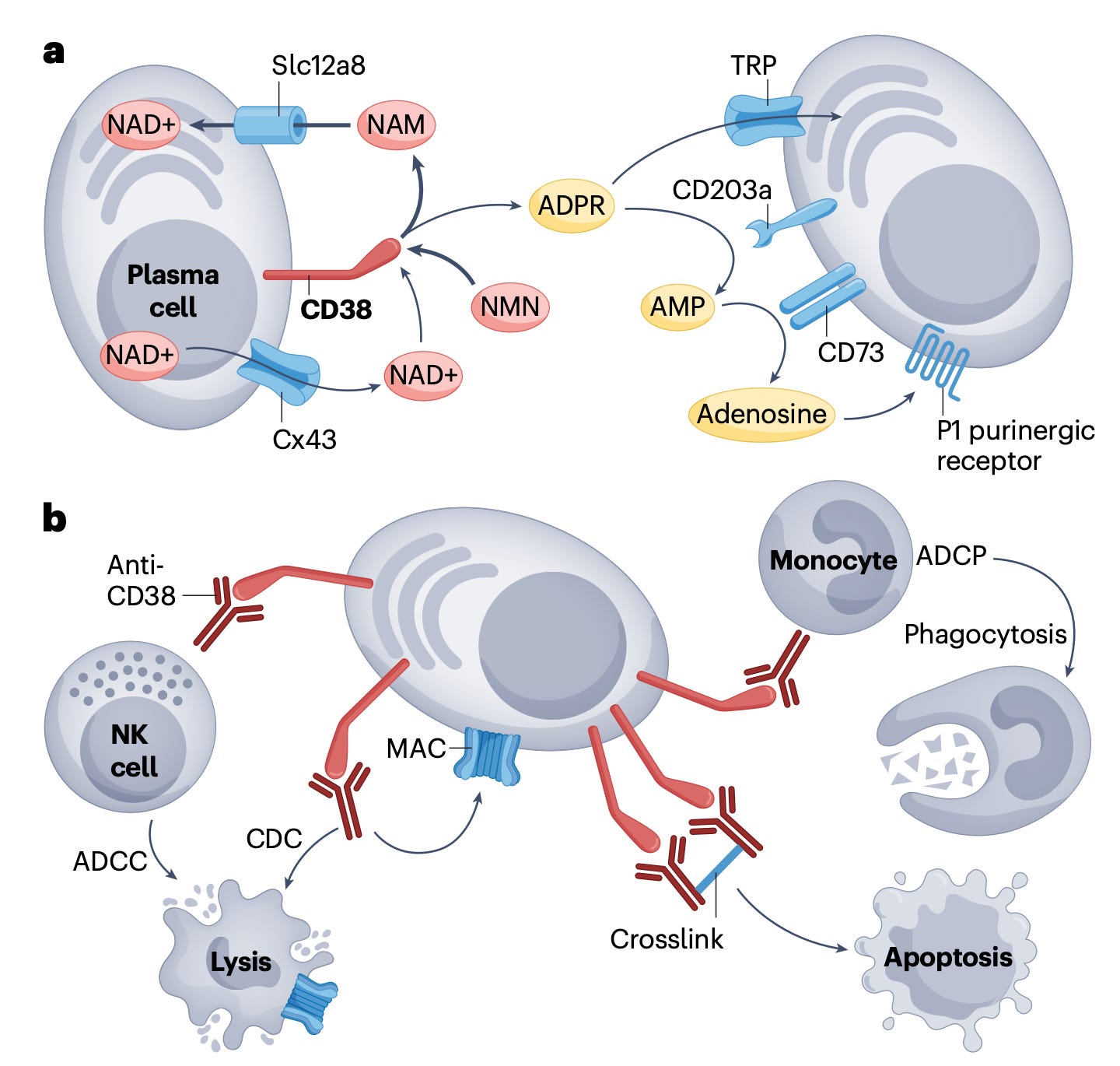
Drs. Böhmig and Budde approached companies that had anti-CD38 therapies and found a small German company called MorphoSys. MorphoSys developed felzartamab, a monoclonal antibody targeting CD38 that was developed specifically for immune-mediated diseases. Anti-CD38 therapies are commonly used in oncology for multiple myeloma, but clinicians have also used these therapies off-label in difficult autoimmune diseases.
In the transplant setting, there was a case where a patient who had been treated with an anti-CD38 therapy for myeloma later underwent a kidney transplant, developed rejection, and the rejection resolved with therapy. That observation helped motivate the proof-of-concept study. MorphoSys supported the study. I later joined a company that licensed felzartamab from MorphoSys. We completed the study and worked closely with the investigators to read out the results.
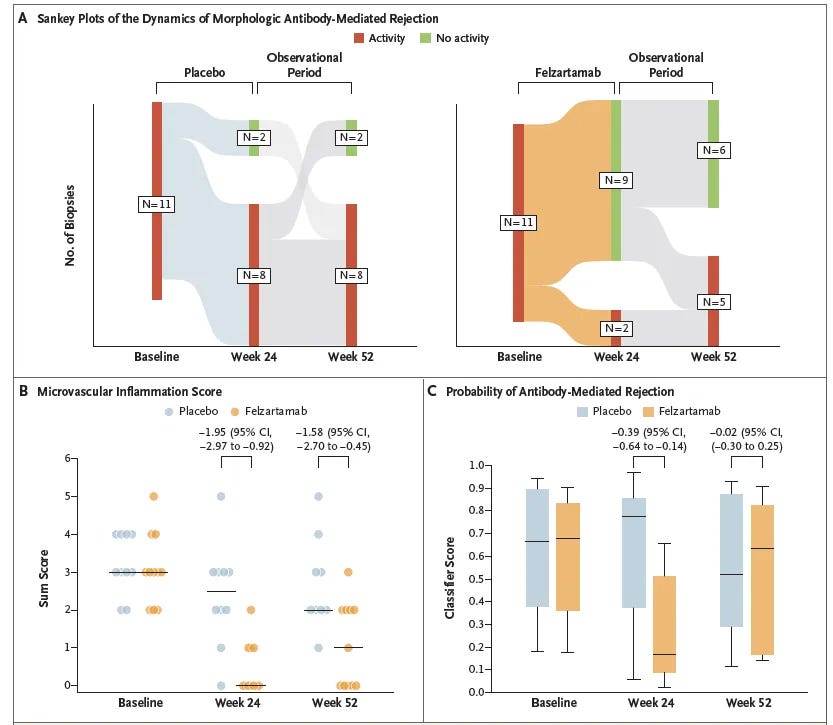
The proof-of-concept study showed a level of AMR resolution that had not been seen before. Roughly 80% of participants in the small Phase 2 study had resolution of AMR compared with about 20% in the placebo group.6 Two-thirds had microvascular inflammation scores down to zero, which had not been seen with other therapies. Microvascular inflammation means inflammation in the tiny blood vessels of the transplanted kidney and is a key histologic feature of AMR.7
What we have learned since is that the biology is more complicated than antibodies alone. Natural killer cells, or NK cells, appear to play a large role too. CD38 is expressed on antibody-producing cells and on NK cells. By modulating or depleting these cells, we saw near reversal of disease activity in molecular tests on tissue samples before and after treatment.
It was a small proof-of-concept study, but other markers were consistent. Molecular activity scores improved. Donor-derived cell-free DNA went to very low levels, suggesting there was no longer active tissue injury. Kidney function stabilized. If this bears out in the Phase 3 study now underway, it could represent a transformative treatment for patients with AMR.8
What does this mean for the field?
Matt: I love hearing stories that begin with someone being uncomfortable with the status quo. That has always driven me in transplant. We are constantly saying we have to do better.
The story Uptal presented started with two physicians who were struggling with AMR and said, “I have an idea. Let’s cooperate with industry and figure out how to make this happen.” The results published in the New England Journal of Medicine from the Phase 2 experience are remarkable and something we should all be excited about.
The reason we need to keep innovating is that until we have an unlimited supply of organs, or we identify a mechanism of tolerance, we have to partner with patients and donor families to increase the lifespan of every graft. For a long time, we could identify AMR and give therapies that might keep it at bay, but they were not durable. They did not leave either the patient or provider feeling rewarded in the effort. Now we may be in a place where we have a potential therapy, and that makes us look more aggressively at early identification.
Mary, why does innovation matter so much for patients?
Mary: Innovation is key. I have had four transplants, and my first was in 1980. That was really the beginning of transplant in many ways. There was not a lot out there. If you had rejection, they threw everything and the kitchen sink at you. They thought something might work, but they did not always know.
For me, financial investment and clinical innovation are not just about survival, freedom, or a normal life. They can be a life-saving miracle. I was rare disease until this past year. When I was diagnosed, my parents were told I had six months to live because they did not dialyze or transplant kids at that point. The reason I am here is innovation. Transplant is here because of innovation. And when we find these problems, we need treatments.
Any final thoughts?
Matt: I want patients to know that the success of transplant is cooperation and partnership. That includes providers, patients, and the tools and technologies we use to ensure the health and longevity of the graft. Communication is key. We all want the same thing. If patients are the captains of their health, let’s grab onto that. If something is out of the ordinary, or if they have a question, they should know there is never a closed sign on the transplant program.
Uptal: I share Matt’s enthusiasm. I am excited about the innovation happening in transplantation and the stronger partnerships across patients, systems, providers, and industry. There is a huge opportunity to maximize the gift of life. I am inspired by people like Dr. Cooper and certainly by Mary, who is a true kidney champion.
Mary: The work that both of you do makes it possible for patients like me to be here. People ask me, “You have had four transplants?” And I always say: transplant works. It has given me a quality of life I never thought I would have. Being sick as a child, until my first transplant, I did not remember what it felt like to feel good.
Transplant gave me everything. It gave me the opportunity to go to school, have a career, get married, and grow old, which I never thought would happen. We need to keep the innovation going so people can keep their kidneys longer and say they have had their transplant 27 years or more, like me. Maybe it took four times to get there, but to me they were all successful.
###
If you're working on early detection, monitoring, or treatment in transplant, we'd love to hear what you're seeing. Leave a comment or pass this along to someone who should see it.
Antibody-mediated rejection, often abbreviated AMR or ABMR, has been described in the transplant literature as a leading cause of late kidney graft loss. Reviews also note that AMR treatment remains heterogeneous because of limited robust trial evidence to guide clinical decisions.
BK virus and cytomegalovirus, or CMV, are viral infections monitored after transplant because immunosuppression can increase infection risk. BK virus is particularly relevant in kidney transplantation because it can affect the transplanted kidney.
Donor-specific antibodies, or DSAs, are antibodies that recognize donor antigens. DSAs are an important risk factor for AMR and graft loss, though not all DSAs are pathogenic.
Donor-derived cell-free DNA, or dd-cfDNA, is a noninvasive blood-based biomarker that can detect allograft injury, including injury associated with rejection, though it is not specific to the exact cause of injury by itself.
Dr. Georg Böhmig:
https://rpt.meduniwien.ac.at/forschung/research-groups/georg-boehmig-md/
Dr. Klemens Budde
https://mrc.charite.de/en/research/buddes_lab
In a randomized Phase 2 trial published in The New England Journal of Medicine in 2024, felzartamab was studied in patients with late antibody-mediated rejection after kidney transplantation. At week 24, morphologic AMR resolution occurred in 9 of 11 patients receiving felzartamab compared with 2 of 10 receiving placebo; the study also reported lower microvascular inflammation scores, lower molecular AMR activity scores, and lower donor-derived cell-free DNA levels in the felzartamab group.
Microvascular inflammation, or MVI, refers to inflammation in small vessels within the transplanted kidney and is a key histologic feature used in diagnosing AMR. The Banff Classification is a widely used international framework for interpreting kidney transplant biopsies and rejection phenotypes.
A Study to Learn More About the Effects and Safety of Felzartamab Infusions in Adults With Kidney Transplants Who Have Antibody-Mediated Rejection (AMR) (TRANSCEND):
https://clinicaltrials.gov/study/NCT06685757
