![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!IXc-!,w_120,h_120,c_fill,f_webp,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F9f7142a0-6602-495d-ab65-0e4c98cc67d4_450x450.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!lBsj!,e_trim:10:white/e_trim:10:transparent/h_48,c_limit,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F0e0f61bc-e3f5-4f03-9c6e-5ca5da1fa095_1848x352.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!NnOt!,w_144,h_144,c_fill,f_auto,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F688fc47b-7202-4a2e-b4f4-fea2b047ab1b_1500x1500.png)

Most patients with chronic kidney disease never know they have it—until it’s too late. But what if you could design a care model that reaches them sooner?
That’s what today’s guests have done. Seth Southwick and Chenlee Condie joined me to share more about Intermountain Health’s Kidney Services program, a six-year effort to reimagine kidney care within one of the country’s largest integrated health systems. In this interview, we discuss:
How Intermountain designed and scaled its kidney services program
Why nurse navigators became the linchpin of their model
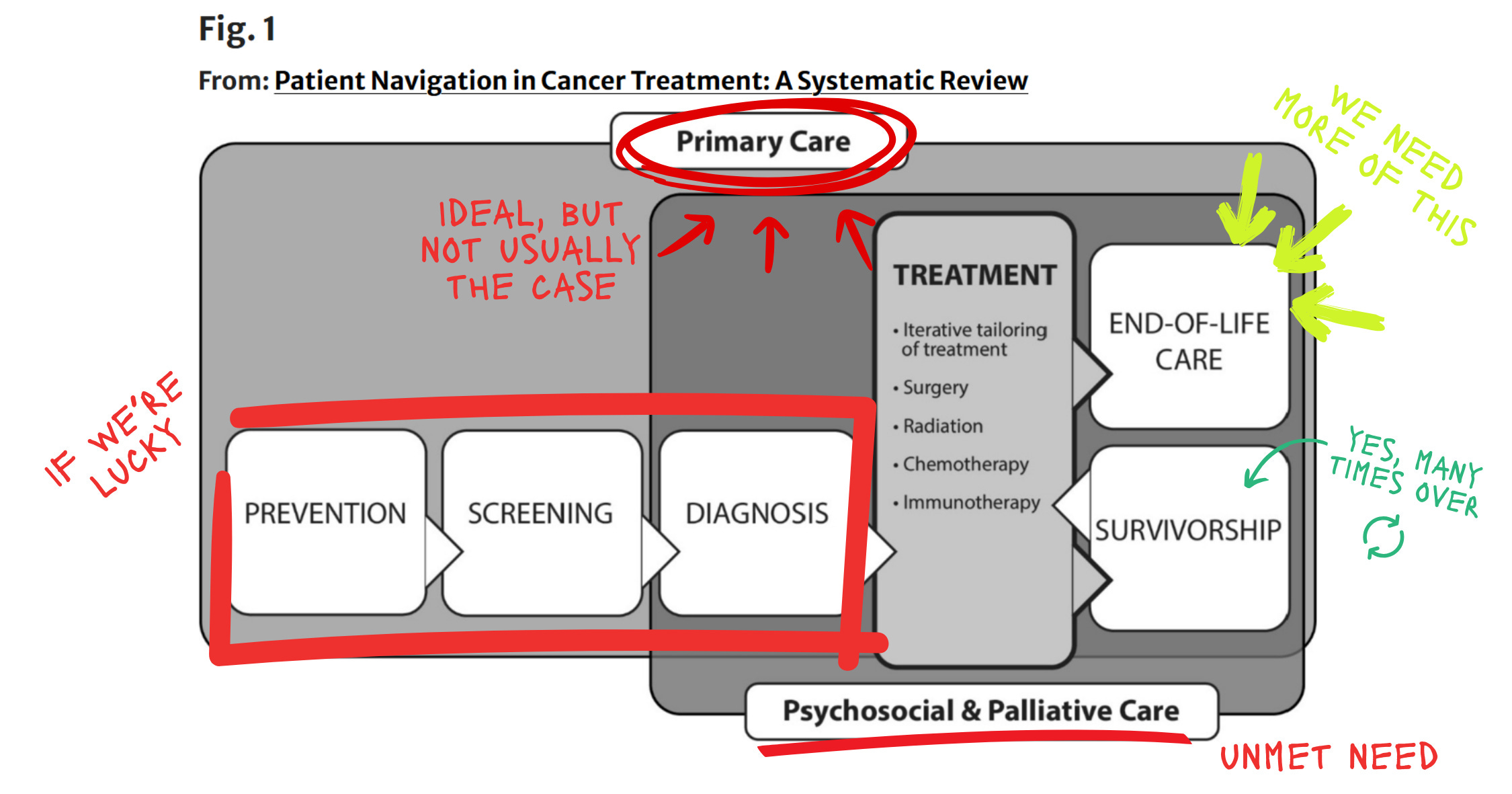
What it takes to shift care upstream—from the ED to primary care
How they grew their nephrology workforce 10x across 7 clinics
Why mission alignment has been essential to their progress
What makes measuring outcomes in value-based care so difficult
And what they’re thinking about next as they transition to Epic
As Seth and Chenlee describe, Intermountain’s program is a product of culture, coordination, and relentless focus on relationships—especially with the patients who need it most. I know you’ll enjoy this inside look at how kidney care is designed, delivered, and scaled at the health system level as much as I did. And in case you missed it, here is the piece on kidney care navigation where this all started.

How did you get into kidney care?
Seth: I’m Seth Southwick, Assistant Vice President of Kidney Services at Intermountain Health. I’ve been in this role for almost five years. I originally fell into kidney care — I was pre-med during undergrad and looking for healthcare experience when some family members in dialysis encouraged me to check it out. I got a job as a dialysis tech, stayed after graduation, and moved into leadership roles over time. Now, I oversee all dialysis and nephrology operations across the enterprise, supporting Chenlee, our physician groups, and all value-based care and comprehensive kidney care efforts.
Chenlee: I’m Chenlee Condie, a nurse by background with 28 years of experience. I got into dialysis after a neighbor suggested it might be easier on my back than hospital nursing — and I came to love the long-term relationships in this field. I’ve been at Intermountain Health since 2001 as a dialysis nurse, kidney transplant coordinator, and manager of various programs. Today I’m Director of Clinical Services for Kidney Services, overseeing nurse navigation, home dialysis, education, and our clinical guidelines.
How did Intermountain Kidney Services (IKS) get started?
Seth: When I joined Intermountain, we were talking about launching an ESCO. Some of our earliest planning — literally on napkins — was focused on reducing emergency department admissions. As we took those first steps, our vision kept expanding. We leaned into our Select Health payer arm, our population health team (formerly Castell), and built from there. Culturally, it was a natural fit with Intermountain’s mission to help people live the healthiest lives possible — which meant moving upstream from dialysis and focusing on CKD care. Our first clinic launched nearly six years ago and it’s grown rapidly since then into multiple markets with physicians, APPs, navigators, and a broader operations team.
Chenlee: I remember being struck when patients starting dialysis would say, “No one told me my kidneys weren’t working.” It was heartbreaking. When I saw this program’s focus on upstream care and closing awareness gaps, it really resonated. Only about 1 in 10 people with CKD even know they have it. This was our chance to change that.
Seth: Intermountain has owned dialysis centers for over 40 years, so we had an existing infrastructure to build on — including financials and expertise. Of course, the last five years haven’t been easy: COVID, inflation, and financial headwinds. But knowing we’re making a difference keeps us going.
How does Kidney Services fit into the broader Intermountain organization?
Chenlee: Intermountain has long held risk contracts with payers. We built this program to bring value-based kidney care to the entire organization. Select Health was a key partner, giving us access to data and analytics to identify and close care gaps. Intermountain’s willingness to invest — especially in our nurse navigator program — has made a huge difference. That one-on-one support empowers patients with knowledge and choices they’ve never had before.
Seth: Intermountain has a track record of being ahead of the curve. We had a medical group before most health systems, and we created Select Health before the “payvider” concept took off. All of that laid the foundation for kidney services— an integrated delivery system, a fully at-risk payer, and strong alignment on mission. But it’s not always easy: we still operate in a fee-for-service world while delivering value-based care, so we often face legacy processes that weren’t built for what we’re doing. Still, kidney is now seen as leading the way across Intermountain.
When does Kidney Services step in? What does that handoff look like?
Chenlee: Our program is well-integrated with primary care. We developed a care process model, published guidelines for providers, and implemented better screening using the Kidney Failure Risk Equation (KFRE), which is now a single order in our EMR. PCPs are empowered to manage early-stage disease, and we recommend referring any patient with over a 3% risk.
Once referred, patients see a nephrologist or APP and then immediately meet with a nurse navigator. The navigator builds that relationship, reinforces what was said in the visit, screens for social needs, and supports patients throughout the entire journey — from slowing progression to understanding transplant and other treatment options.
Seth: We have a small but tightly aligned leadership team. I work in dyad with Dr. Anitha Vijayan, and we lead the enterprise effort. We’re integrated across population health, the payer, IT, transplant, and clinical service lines. We only began employing nephrologists six years ago — we started with two MDs and four APPs and now have 23 nephrologists across seven clinics. Growth has been fast.
Chenlee: Our navigator team has grown too— from three to eight. We now aim for one navigator per physician. When we budget for a new nephrologist, we also budget for a navigator.
Tell us more about the navigator program— what they do, how it started, and what makes it work.
Chenlee: When we first launched, we proactively identified patients using analytics and had our navigators reach out to PCPs to facilitate referrals. Our PCP community was very receptive. Once referred, navigators meet with the patient right after their provider visit — they explain what was discussed, answer questions, give them a direct contact number, and follow up to ensure continuity.
This relationship is crucial. Patients with CKD often feel fine, so it’s easy to deprioritize follow-up care— until it’s too late. Our navigators track patients, re-engage them if they miss appointments, and help prepare them for whatever path they choose: transplant, dialysis, or medical management. They're also instrumental in social needs screening and education.
Seth: Our navigators genuinely care. They go above and beyond — and they stay. We’ve had virtually no turnover in six years. They’re all former dialysis nurses who deeply understand the journey and want to make it smoother for others.
What outcomes are you seeing?
Chenlee: Our optimal start rate in 2021 was 20%. Now it’s 70%. That means 70% of our patients don’t crash into dialysis — they start in a planned, informed way. Among those, 50% received a preemptive transplant. We’re also tracking improvement in guideline-directed medical therapy, including use of ACE/ARBs and SGLT2s. It’s ongoing work, but the progress is real.
Seth: It hasn’t been easy. Intermountain has to weigh things like buying an MRI, which breaks even in months, versus opening a new nephrology clinic, which may take years to break even. But our outcomes and alignment with the mission help make the case. Financial performance has been strong overall.
What have been the biggest hurdles?
Chenlee: Getting support for non-revenue-generating roles like navigators is tough. We rely on outcomes like optimal starts to demonstrate their value. Accurate data is another challenge — making sure we have the right resources and validation in place.
Seth: Inertia is a big one. Intermountain’s roots are in acute care, and changing mindsets and systems is difficult. We also face turnover in key roles — just when someone understands kidney care, they move to a new department. And building the right tools into our EMR has been a huge lift, especially now with the transition to Epic.
What’s top of mind for the next 12–24 months?
Seth: Epic, first and foremost — ensuring we don’t lose momentum during the transition. Beyond that, we’re focused on scaling. In a world full of data and AI, we’re asking how to preserve the human-to-human connection that matters so much. How do we scale relationships? That’s what keeps me up at night.
Chenlee: A patient recently said after a visit, “I wish I’d known this 15 years ago.” That stuck with me. We have to reach people earlier. Technology helps, but we can’t lose the human element. Relationships are what make the difference.
Final thoughts for us?
Seth: It’s a team effort. The quarterback can’t win without blockers and receivers. We’ve built something unique around people — patients and caregivers — and we’re really proud of that.
My thanks to Seth and Chenlee for joining us. For more on the importance of early intervention, policy innovation, and proactive collaboration to transform the management of kidney disease and optimize patient outcomes, check out this 2024 article in AJMC. For more from Seth on the power of leveraging community partnerships and advanced data analytics, check out this interview (also from AJMC’s Kyle Munz). For a ground-level view of where this all started, check out this 2020 abstract on ML-driven CKD care navigation from Titte Srinivas, Ray Morales, Suji Lee, and Michael Phillips.
