![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!IXc-!,w_120,h_120,c_fill,f_webp,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F9f7142a0-6602-495d-ab65-0e4c98cc67d4_450x450.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!lBsj!,e_trim:10:white/e_trim:10:transparent/h_48,c_limit,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F0e0f61bc-e3f5-4f03-9c6e-5ca5da1fa095_1848x352.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/$s_!NnOt!,w_144,h_144,c_fill,f_auto,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F688fc47b-7202-4a2e-b4f4-fea2b047ab1b_1500x1500.png)

On this International Women’s Day, in the first week of Kidney Month, today’s recap feels like the right lens for what’s unfolding. CMS is pushing upstream through the ACCESS model. HRSA is modernizing transplant governance amid a shifting donor landscape. AI is moving from pilots into real clinical workflows. Precision tools are redrawing long-held diagnostic lines. From dialysis to transplant to early risk detection, the architecture of kidney care is being adjusted from the ground up.
This month’s news begs a bigger question: what was our kidney care system made for? In the Barbie film, Billie Eilish’s “What Was I Made For?” becomes a quiet reckoning about purpose. The title feels like a fitting frame now. Was this system built to manage late-stage failure, or to intervene earlier? To reward volume, or to align around outcomes? To operate in silos, or to treat cardiovascular, kidney, and metabolic disease as the connected reality they are?
Let’s get into it.
Thank you all for being part of Signals. Please take a few minutes to share what you’d like to see from us in 2026 in our annual reader survey.1
What’s Inside
News: ACCESS model details, OPTN modernization update, DCD expansion, HHD innovation, major industry bets, Ivenix recall;
Research: Finerenone Phase 3 data, precision transplant tools, AI in workflow, upstream CKD screening gains
Community: RPA preview, AI-ready practices, dialysis innovation debate, CKM unification voices, transplant stories
Events: World Congress of Nephrology, Renal Physicians Association, NKF Spring Clinical Meetings, ANNA National Symposium, Columbia CKM, and more
Jobs: Ardelyx, Travere, Strive, Monogram, Takeda, Boehringer, Vertex, Revalia, Trestle, CVS Health, Getinge, Natera + dozens more on jobs.signalsfs.com…

2026 Reader Survey!
Help shape the future of Signals. We’re expanding across research, data, community, and new tools for the kidney and CKM space. Take 5 minutes to share what would be most valuable to you here. Ten people will receive a $50 digital gift card as a thank you.2
News
POLICY & REGULATORY
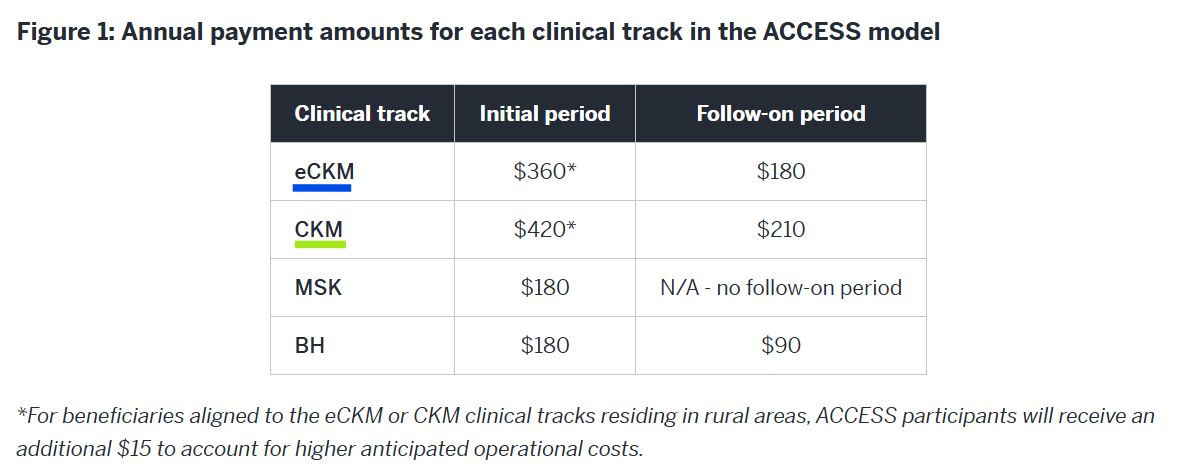
CMMI’s new ACCESS model introduces outcome-aligned payments for early CKM care. The 10-year voluntary model allows organizations to participate in four tracks, including early cardio-kidney-metabolic (eCKM) and CKM (CKD stage 3a or 3b), shifting Medicare FFS reimbursement from volume to outcome-aligned payments (OAPs). For the CKM track, participants can receive $420 per beneficiary in the initial 12-month period and $210 in follow-on years, with an additional $15 rural adjustment. Payments are tied to clinical improvement thresholds and reduced duplicative services, with semiannual reconciliation and potential downward adjustments if fewer than 50% of patients meet outcome targets. CMS will also introduce a co-management payment (~$30 per beneficiary, quarterly) for care coordination. Advocates say the model signals a serious federal push to fund technology-enabled, accountable upstream CKM management rather than waiting until dialysis. Author’s note: I’ll be writing about this in more depth soon, with performance scenarios tailored for both neph practices and tech vendor partners focused on e/CKM. As a reminder, to be considered for the model’s first performance period beginning July 5, 2026, applications must be submitted via the Participant Portal by April 1, 2026. Applications received after this date will be considered for a January 1, 2027 start.
HRSA’s February update outlines continued modernization of the OPTN, focused on governance reform, technology infrastructure, transparency, and oversight across the transplant system. Key developments include launch of a new OPTN 411 call line (handling 300+ calls in its first month), expanded financial assistance for living donors with income limits removed, addition of 144 new volunteers to OPTN policy committees, rollout of a government-managed Transplant Data Services (TDS) platform, a new Ventilated Patient Form to improve OPO referral visibility, and forthcoming quarterly public reports on transplant center registration fees. The modernization effort signals continued federal pressure to realign transplant infrastructure with current clinical and public health realities.
Fresenius Kabi recalled certain Ivenix large volume infusion pumps after a software issue that can delay or interrupt therapy and misreport battery life, prompting the FDA to classify the action as Class I, its highest risk level. The issue has been linked to two serious injuries, and the company is directing providers to update to the latest software version. The recall follows multiple prior safety actions and a 2024 FDA warning letter related to the Ivenix platform, which Fresenius acquired in 2022 for $240 million.
Healthy People 2030 is calling renewed attention to dialysis vascular access, as central venous catheter use rises and mortality worsens. Despite arteriovenous fistulas (AVFs) being the gold standard, nearly 85% of new dialysis patients start with a catheter, which carries a fourfold higher mortality risk. USRDS data show catheter rates climbing post-pandemic, alongside Medicare reimbursement pressures and Medicare Advantage policies that may delay timely access creation. Advocates argue that reaching catheter reduction goals will require payment reform, stronger support for vascular access centers, and renewed focus on infection prevention. (Healio, H/t Terry Litchfield)
INDUSTRY MOVES
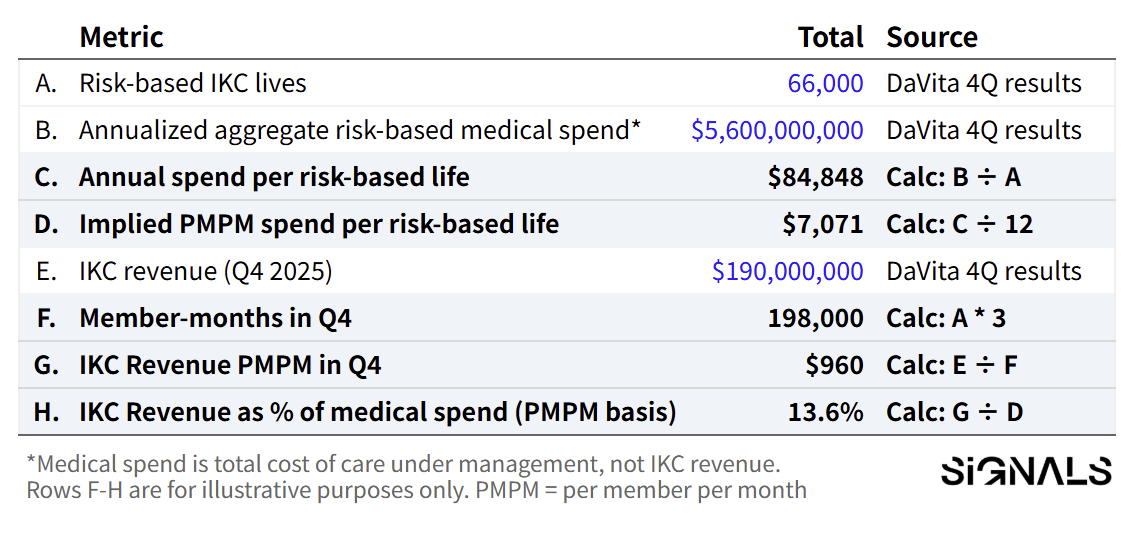
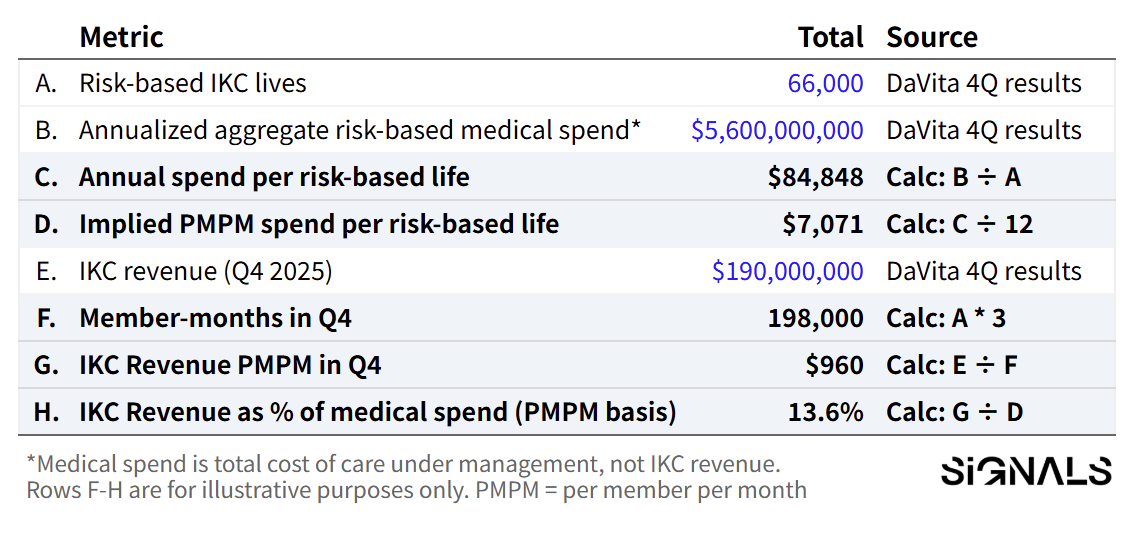
DaVita announced a strategic investment in Elara Caring to co-develop a kidney-specific home-based care model, signaling a push beyond the dialysis clinic and into coordinated in-home support. The partnership pairs DaVita’s risk-based care arm (IKC), which turned profitable in 2025 and now manages roughly $5.6B in annualized medical spend, with Elara’s multistate home health platform. The goal: reduce preventable hospitalizations and lower total cost of care by building the operating layer around kidney patients at home. It’s a bet that value-based economics can fund the next phase of at-home kidney care. Read my full analysis here.
CareDx announced VANTx™, a cloud-native, AI-powered clinical data and analytics platform built on its large-scale longitudinal transplant datasets, unveiled at the 2026 Precision Medicine World Conference. The platform enables secure cohort analysis across patient timelines to support clinical research, real-world evidence generation, and transplant program insights, integrating de-identified molecular, clinical trial, EMR, and remote monitoring data. Built on Databricks and leveraging Llama 3 and proprietary predictive models (KOAR, SHORE, ALAMO, MAPLE), VANTx is designed to help transplant centers and pharma partners generate actionable insights across kidney, heart, lung, and liver transplantation. (H/t Jenny Sato, Hal Gibson)
SeaStar Medical reported post-approval data showing its selective cytopheretic device (Quelimmune) was safe and may benefit children with life-threatening sepsis-associated AKI requiring kidney replacement therapy. In the first 21 pediatric patients treated under its FDA humanitarian device exemption, 90-day survival was 71%, with no device-related adverse events reported. The device, which works alongside CRRT to modulate hyper-inflammation, is currently the only FDA-approved therapy for this critically ill pediatric population, with additional studies ongoing in both children and adults. (H/t Kevin Chung)
Cedars-Sinai performed its first fully robotic kidney transplant, joining a small group of U.S. centers offering robot-assisted implantation for recipients. The minimally invasive approach uses smaller incisions, which may reduce pain, infection risk, and recovery time, particularly for patients with higher BMI who face greater wound complication risk. The program aims to expand robotic procedures to as many as 40% of kidney transplants over the next 3–5 years, while emphasizing that patient selection remains individualized.
Digital health M&A wave gains momentum in 2026. MedCity News reports a sharp uptick in targeted acquisitions, including Sword Health’s $285M purchase of Kaia Health and OpenAI’s $60M acquisition of Torch, as digital health companies seek scale, AI capabilities, and stronger payer leverage. Investors expect continued consolidation, particularly in primary care, post-acute care, ancillary services, revenue cycle management, imaging/radiology, robotics, and consumer health. With IPO markets uncertain, M&A may become the dominant exit path this year.
DATA & INFRASTRUCTURE
Springer Nature and GlomCon launch Rare Kidney Diseases journal. Springer Nature will publish Rare Kidney Diseases, a fully open access journal from the GlomCon Foundation dedicated to research and innovation in rare and complex kidney disorders. Submissions are expected to open in early 2026, with a focus spanning clinical insights, pathology, and AI applications.
AST pushes for iBox biomarker qualification at Congressional briefing. The American Society of Transplantation hosted a Capitol Hill briefing focused on patient-centered innovation in transplant immunosuppression, highlighting the burden of current therapies and the need for safer options. A key priority was FDA qualification of the iBox composite biomarker, developed through the Transplant Therapeutics Consortium, as a reasonably likely surrogate endpoint for long-term kidney graft survival. If qualified under the accelerated approval pathway, iBox could modernize transplant trial design and speed access to new therapies while maintaining scientific rigor. Watch it here. (H/t Kevin Fowler)
Eledon’s Tegoprubart pilot study in islet transplantation completed enrollment (N=12), with 7 patients achieving sustained insulin independence and the earliest participant remaining insulin-free for up to 18 months. The tacrolimus-free immunosuppression regimen has been well tolerated with no observed toxicity, and a related study in patients with type 1 diabetes and chronic kidney disease is expected to open soon (LinkedIn, h/t Piotr Witkowski)
Dr. Adebowale Adebiyi at the University of Missouri received a $2.8 million NIH grant to study a newly identified contributor to acute kidney injury in premature infants. His research suggests overactivation of voltage-gated sodium (NaV) channels in kidney blood vessels may restrict oxygen delivery during injury, worsening organ dysfunction. The project will explore how nitric oxide interacts with these channels and whether targeting this pathway could restore blood flow and protect kidney function in vulnerable NICU patients.
Research
THERAPEUTICS
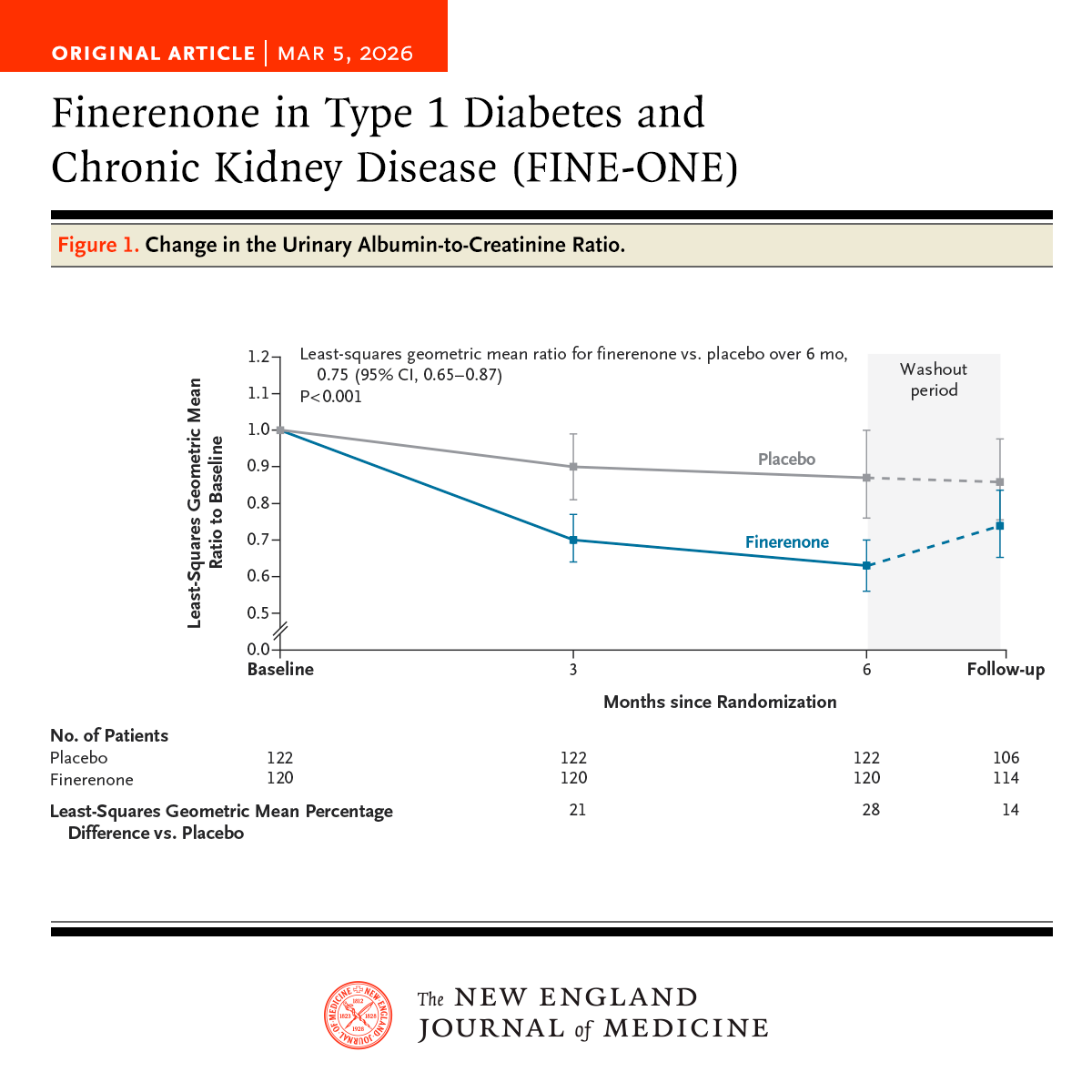
Finerenone shows first positive Phase 3 data in Type 1 diabetes and CKD since 1993. In a Phase 3 trial published in NEJM, finerenone reduced UACR by 34% over six months in adults with Type 1 diabetes and CKD, compared to a 12% reduction with placebo — a 25% greater reduction overall (P<0.001). eGFR declined modestly at 6 months (–5.6 vs –2.7 ml/min/1.73m²), but values approached baseline after washout, suggesting a hemodynamic effect. Hyperkalemia occurred in 10.1% of finerenone patients vs 3.3% with placebo. This is the first positive Phase 3 trial in this population since the Captopril trial in 1993, and it uses a bridging-biomarker approach to extrapolate albuminuria reductions to long-term outcomes based on prior Type 2 diabetes data. (H/t Robert Lawatscheck, MD, PhD)
Finerenone reduces heart failure hospitalizations within months, with kidney benefits accruing over time. A participant-level analysis of FIDELITY and FINEARTS-HF published in JACC found that heart failure hospitalization was the earliest event prevented with finerenone. In FIDELITY, sustained statistical significance for HF hospitalization emerged at ~6 months, compared with ~10 months for the composite kidney outcome. In FINEARTS-HF, HF hospitalization reached significance as early as 0.9 months. The findings suggest that finerenone delivers near-term cardiovascular risk reduction, while kidney protection becomes more apparent with longer follow-up, reinforcing the case for earlier implementation in high-risk CKM patients. (H/t Brendon Neuen)
PRECISION MEDICINE
KPMP biopsy data reveal diagnostic blind spots in diabetic CKD. In a preprint from the Kidney Precision Medicine Project, only 56% of participants enrolled as diabetic kidney disease (DKD) had biopsy-confirmed diabetic nephropathy, underscoring substantial diagnostic heterogeneity. Molecular profiling showed immune and inflammatory pathway upregulation and oxidative phosphorylation downregulation in confirmed diabetic nephropathy, alongside more severe fibrosis and tubular injury. A clinical-biomarker model (age, HbA1c, UACR, KIM-1, sTNFR1) predicted biopsy-confirmed diabetic nephropathy with an AUC of 0.82 and was associated with CKD progression in CRIC (HR 1.48 per 10% higher predicted probability). The findings strengthen the case for precision diagnostics beyond clinical labels alone.
iBox accurately predicts graft loss in African American transplant recipients. In a multicenter North American preprint study of 3,588 kidney transplant recipients, including 866 African American patients, the iBox prognostication system showed similar discrimination for graft loss across groups (C-index 0.81 vs 0.83; p=0.25) with no significant interaction by race. Although African American recipients had higher baseline risk and a greater 7-year hazard of graft loss (HR 2.14; p<0.001), calibration and overall performance remained robust up to 7 years post-evaluation. The findings support iBox as a relevant surrogate endpoint across diverse transplant populations. (H/t Amanda Klein)
Microvascular inflammation extends beyond classic antibody-mediated rejection. A review by Alexander Loupy and colleagues highlights that microvascular inflammation (MVI) includes DSA-negative and C4d-negative forms now recognized in updated Banff criteria and linked to worse graft outcomes. Donor-derived cell-free DNA is emerging as a leading noninvasive marker of active injury, and therapies such as CD38-directed agents are under study. The authors call for integrating histology, molecular diagnostics, and AI tools to better classify and treat alloimmune injury. (H/t Alex Loupy)
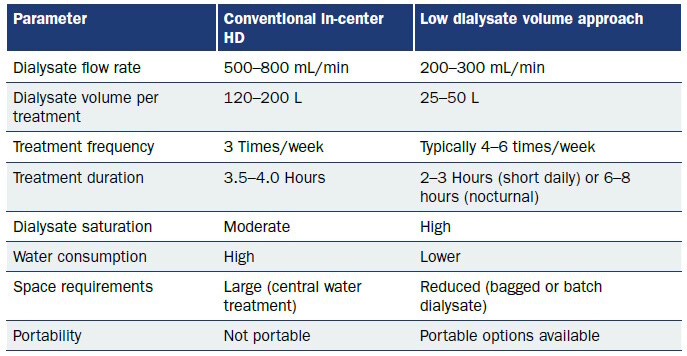
A new review in Kidney News outlines rapid automation and design advances across seven FDA-approved home hemodialysis (HHD) machines, highlighting features such as on-demand dialysate production, cloud-based monitoring, automated saline flushes, and enhanced needle dislodgement detection. Despite rapid device innovation, only 0.4% of incident kidney failure patients initiate HHD in the U.S., underscoring that technology alone hasn’t shifted modality adoption.. (H/t Osama El Shamy)
Figure: Comparison of conventional HD with the low dialysate volume approach
AI & REAL-WORLD EVIDENCE
Clinical Kidney Journal lays out a roadmap for AI integration in nephrology.
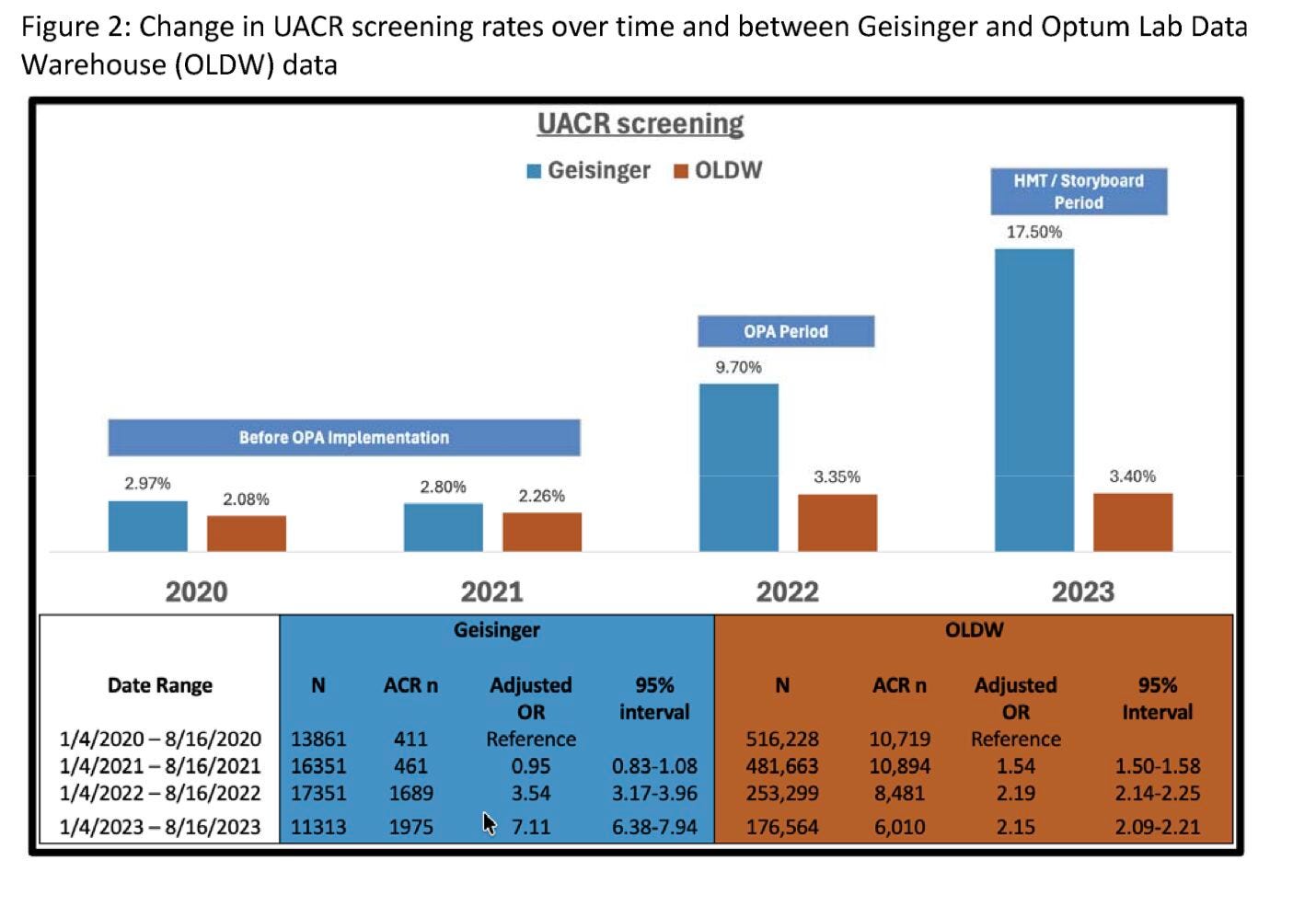
A new state-of-the-art review outlines how AI is moving from pilot projects to clinical integration across AKI, CKD, dialysis, and transplantation. Predictive AKI models, CKD risk stratification tools, AI-enabled dialysis management, and transplant platforms such as iBox are highlighted as leading use cases, though workflow integration and real-world validation remain uneven. The authors flag data bias, interpretability, and regulatory uncertainty as key barriers, and point toward multimodal data integration, reinforcement learning, and digital twins as the next frontier in precision nephrology. (H/t Davide Garrisi)A new preprint shows that simple EHR design changes dramatically improved albuminuria screening in patients with hypertension. At Geisinger, UACR testing rose from ~3% in 2020–2021 to 9.7% in 2022 and 17.5% in 2023 after implementing two clinical decision support tools, compared to only ~3% in control health systems. An initial advisory increased testing roughly 3-fold, while a redesigned health maintenance prompt drove ~6-fold improvement from baseline. The findings suggest that thoughtful CDS design, not just guideline awareness, can meaningfully close upstream CKD screening gaps. (H/t Alex Chang)
AI-triggered interventions reduced short-term hospitalizations in ESKD. A Medicare- and EMR-linked analysis in NEJM Catalyst evaluated AI models that flagged dialysis patients at risk of hospitalization within 7 days for fluid or infection-related events. Among 10,294 patients and 83,928 risk scores, AI-triggered case reviews were associated with an 8% reduction in the odds of hospitalization. The effect was strongest in patients with moderate-to-high risk scores and not significant in the highest-risk group. The findings suggest targeted, workflow-integrated AI may help bend near-term admission risk in value-based kidney care settings.
EPIDEMIOLOGY
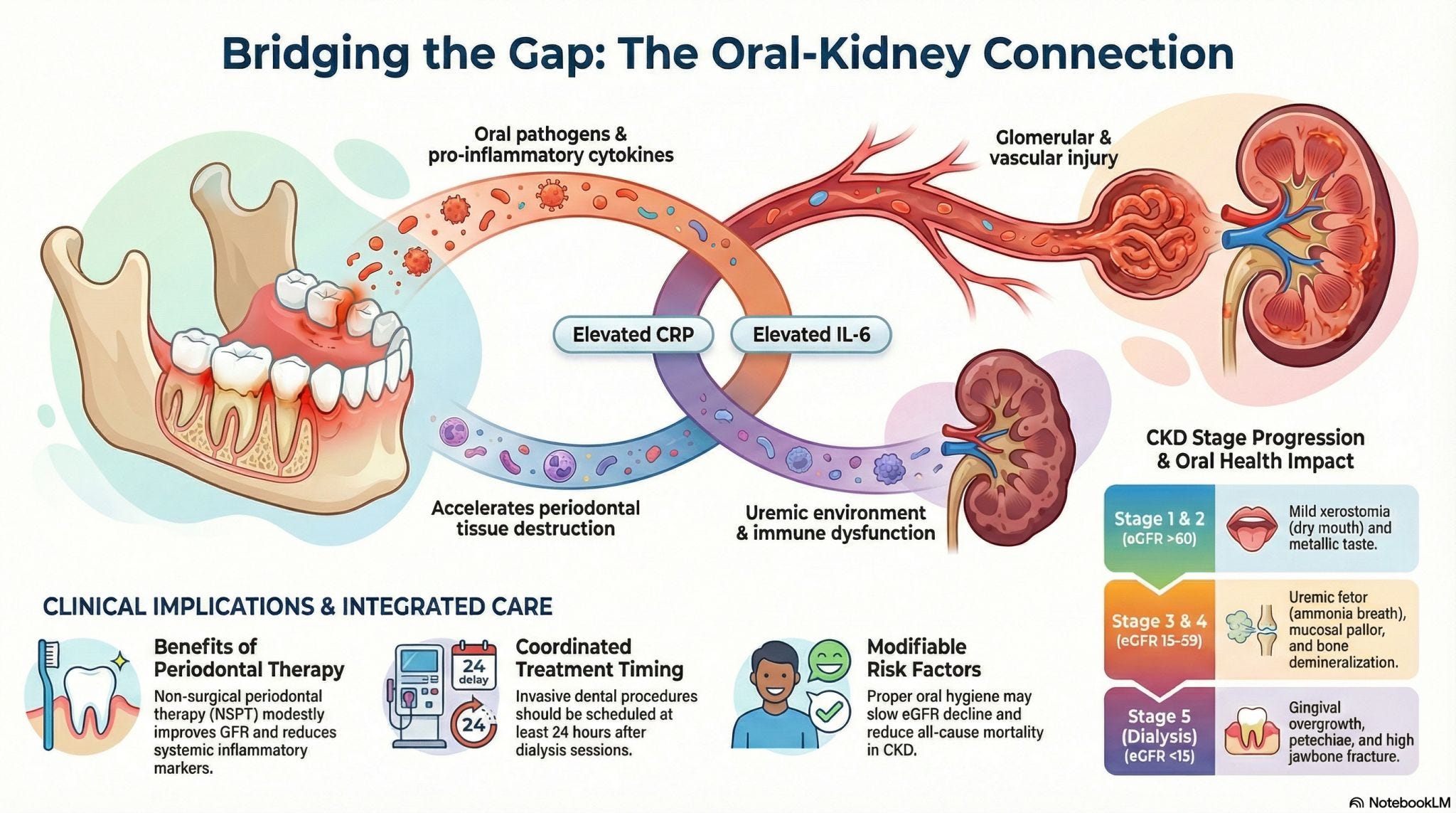
Oral disease tracks closely with CKD progression and systemic inflammation.
A BMC Nephrology narrative review synthesizing observational studies and trials finds that periodontal disease severity rises alongside CKD stage, with higher DMFT scores and clinical attachment loss correlating with lower eGFR and elevated CRP and IL-6. Non-surgical periodontal therapy modestly improves inflammatory markers, though renal outcomes remain mixed. The authors argue oral health is a measurable, modifiable contributor to CKD progression and call for integrating dental assessments into routine nephrology care, particularly in low-resource settings where fragmentation is most pronounced. (H/t Prakash Gudsoorkar)
A review in Nature Reviews Nephrology highlights how social determinants of health (SDoH) shape acute kidney injury (AKI) risk and outcomes worldwide. Factors such as socioeconomic status, race, education, environmental exposure, climate change, and conflict influence AKI incidence, recognition, access to care, and long-term outcomes, with disparities widening in low-resource settings. Pediatric populations face unique vulnerabilities, and gaps in data further limit targeted intervention. The authors argue that reducing AKI burden will require policy reform, interdisciplinary strategies, and alignment with broader public health and Sustainable Development Goals to address structural inequities driving disease risk. (H/t Rolando Claure Del Granado)
A large study in Nature Communications Medicine found that COVID-19 infection is associated with significantly higher kidney risk compared to influenza. In more than 3 million working-age adults, COVID-19 was linked to increased rates of acute kidney injury, chronic kidney disease, end-stage kidney disease, and glomerular disease, while influenza showed no significant association with CKD or ESRD. AKI risk was highest in the short term, while CKD risk persisted over time. The findings support closer kidney monitoring after SARS-CoV-2 infection.
TRANSPLANT TRENDS
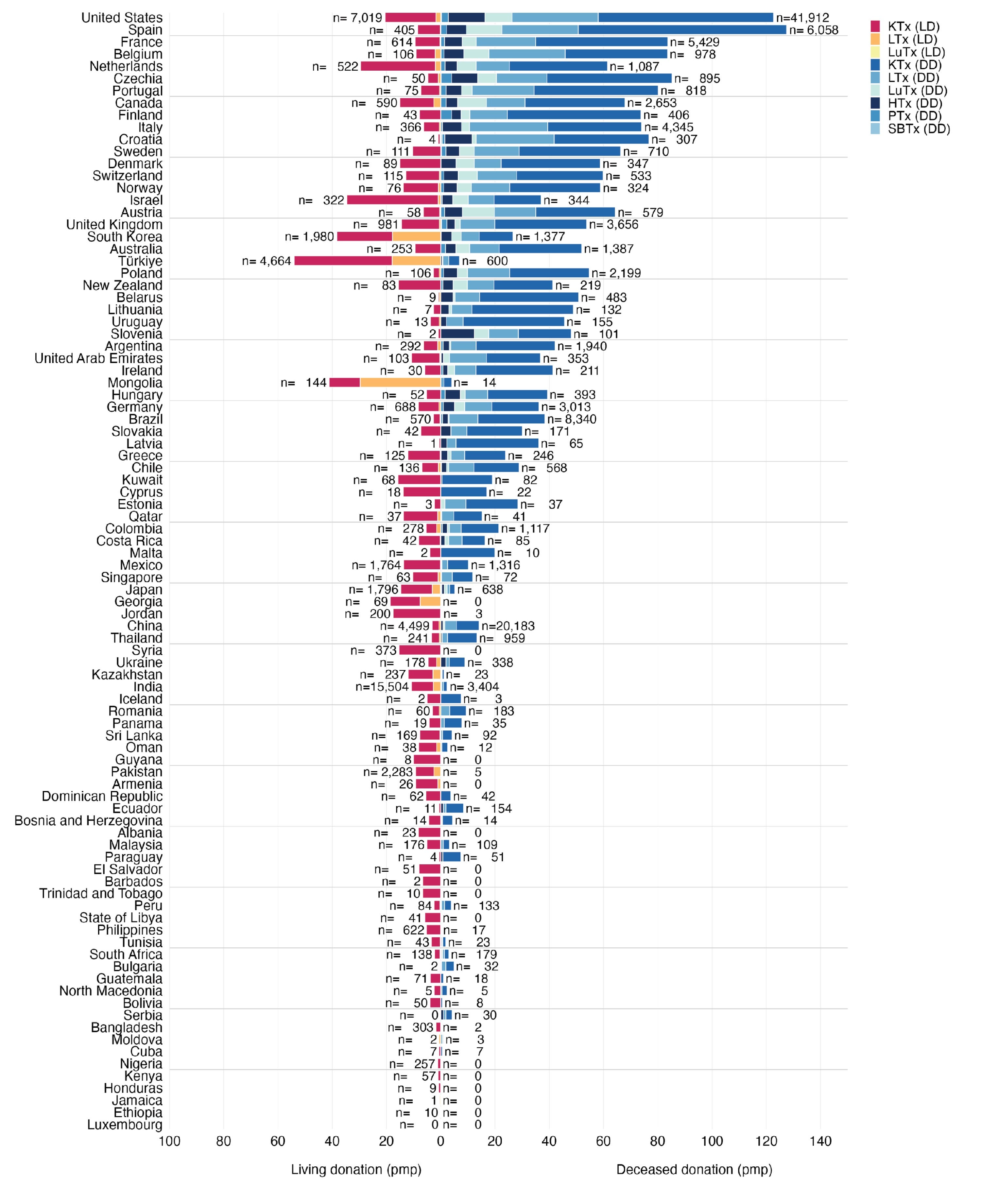
Global transplants hit record high in 2024, but access gaps persist. The Global Observatory on Donation and Transplantation reports 173,727 solid organ transplants worldwide in 2024, a 2% increase from 2023 and the highest number ever recorded. Growth was largely driven by deceased donation, with donations after circulatory determination of death accounting for 28% of all deceased donor activity (47,180 total deceased donations). Despite progress, major geographic disparities and ongoing organ shortages remain central global challenges.
DCD donation continues to expand in the U.S. A research letter in JAMA reports growing use of donation after circulatory death (DCD) as transplant programs respond to persistent organ shortages. Although DCD organs carry higher risks of dysfunction and require more complex recovery logistics than donation after brain death, technological advances and mounting demand have driven increased adoption. The findings highlight DCD as a key lever for expanding the deceased donor pool in the U.S.
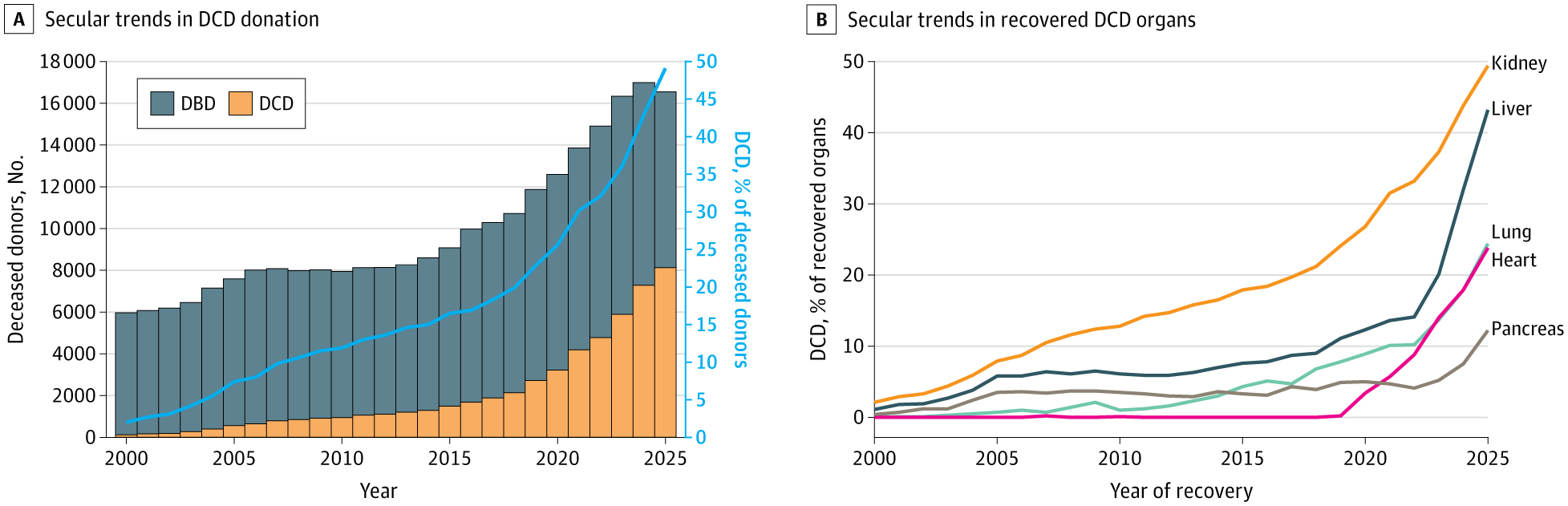
A companion JAMA perspective piece traces the broader evolution of deceased organ donation, from the 1968 Uniform Anatomical Gift Act to the modern transplant system — offering historical context for how today’s DCD expansion fits into decades of policy and infrastructure development. (H/t Aleah Brubaker & Gabe Schnickel)
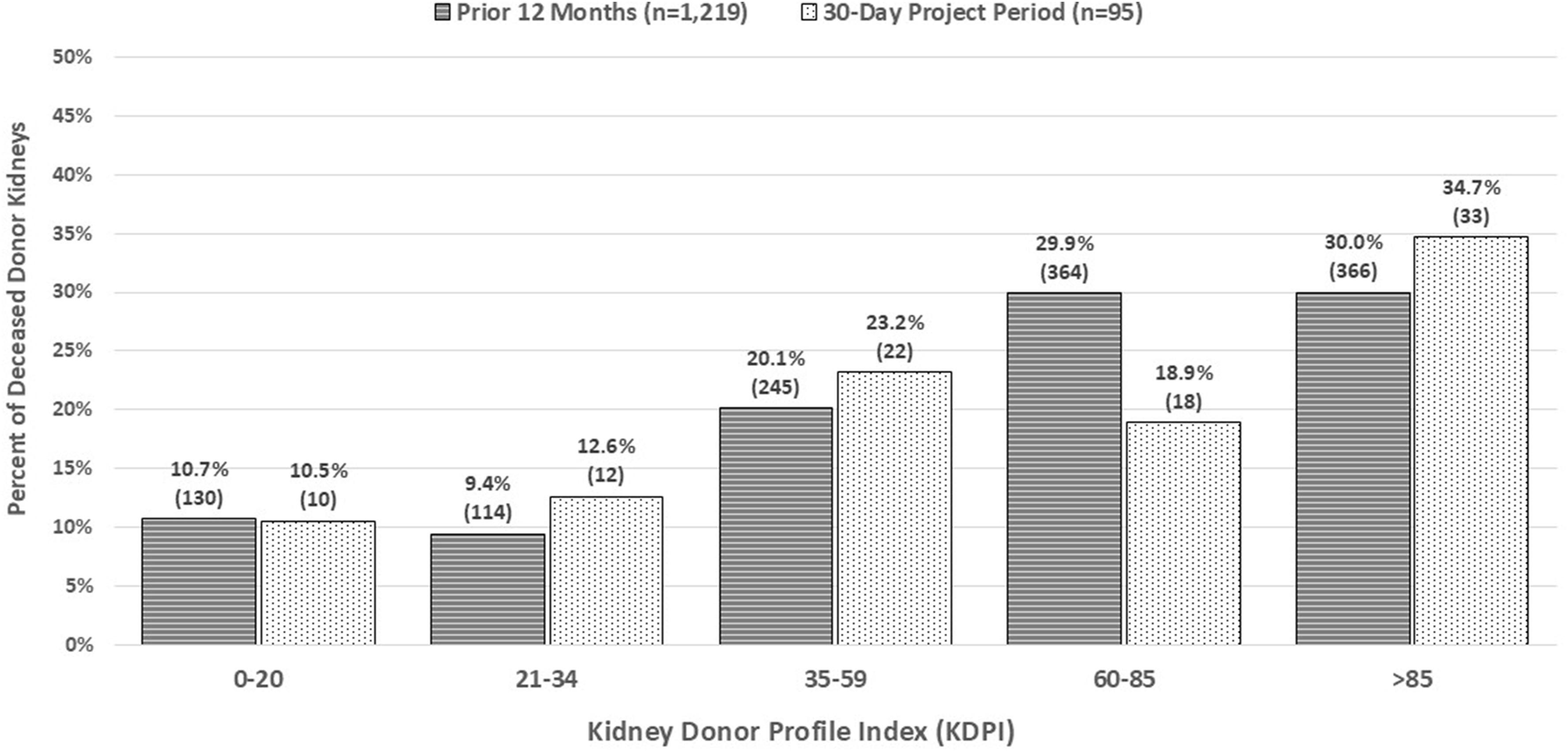
A prospective study in American Journal of Transplantation found that eliminating allocation out of sequence (AOOS) for 30 days increased kidney nonuse. When one OPO (New England Donor Services) strictly followed the national match-run without rescue pathways, nonuse rose from 29.1% to 43.2%, particularly among higher KDPI (more medically complex) kidneys. An estimated 13 additional kidneys might have been transplanted during the study month if prior utilization rates had held. The findings suggest that removing AOOS without a standardized national rescue alternative may increase organ wastage and highlight the need for transparent, policy-driven solutions for hard-to-place kidneys. (H/t Alex Glazier)
Patients favor flexibility in automated peritoneal dialysis prescriptions. In a national survey of 203 people on automated peritoneal dialysis (APD), most respondents reported starting PD at 7 days per week (73%), yet preferences leaned toward more flexible, incremental approaches that reduce treatment burden. Incremental APD options such as fewer weekly sessions, shorter cycler time, or eliminating daytime dwells were ranked based on perceived impact on quality of life. The findings reinforce that incremental PD is not just clinically viable but aligned with patient-centered care, emphasizing life participation alongside adequacy metrics. (H/t Michael Spigler)
Community

INNOVATION MILESTONES
Roivios enrolls first European patient in GRADIENT pivotal study. The GRADIENT trial (NCT07017933) evaluating the JuxtaFlow® Renal Assist Device has enrolled its first patient in Europe, marking a key milestone for the company and its partners at American Heart of Poland. The study is testing whether perioperative use of the device can help sustain or enhance kidney function during high-risk procedures. Congrats, team!
ARPA-H launched ADVOCATE, a new “agentic AI” program aimed at delivering autonomous specialty heart failure care to address clinician shortages, with 46% of U.S. counties lacking a cardiologist. The initiative seeks FDA-authorized AI systems that can provide direct patient care, prescribe medications, integrate with EHRs and wearables, and operate under a novel supervisory AI oversight model. If successful, ADVOCATE could create a regulatory and deployment blueprint for AI-enabled specialty care beyond cardiology, with projected savings of $50B annually. (H/t Haider Warraich)
Blake Madden spotlights Arbital Health’s “Actuarial AI” for VBC. In a new Hospitalogy deep dive, Blake Madden highlights how Arbital Health is building a real-time actuarial operating system for risk-bearing organizations. Its Merlin AI assistant integrates contract logic, claims data, and predictive models into auditable next-best actions built for actuaries and finance leaders. The argument: VBC struggles less from vision and more from missing infrastructure. I think that’s a message many of my VBC readers can relate to (see our recent report here).
A Q&A in Healio highlights the University of Washington’s inpatient “Kidney-Heart” service, a specialized cardio-nephrology model for patients with complex cardiovascular-kidney-metabolic disease. In its first 2.5 years, patients treated under the service had lower rates of AKI dialysis (36.7% vs. 42%) and mortality (16.5% vs. 25%) compared to a prior general nephrology cohort. The program embeds nephrologists with cardiac expertise directly into cardiology and cardiac surgery teams to improve early diuretic management and interdisciplinary coordination. Leaders say the model is feasible with sufficient patient volume and institutional support, and are now expanding into a multidisciplinary outpatient clinic.
PROFESSIONAL DEVELOPMENT
Katie Kwon outlines what to expect at this year’s RPA Annual Meeting (April 16–19, Atlanta), including a new AI-Ready Nephrology Practice certificate, clinical research programming for private practices, and policy discussions with MedPAC Chair Dr. Michael Chernew. The agenda blends practical clinical updates with candid conversations on payment, workforce, and practice management. Will I see you there? Register here.
ASN launches AI-focused podcast for nephrology leaders. The American Society of Nephrology has introduced Rewired: Navigating AI’s Role in Kidney Health, hosted by Karandeep Singh and Navdeep Tangri. The first episode explores generative and agentic AI and how these technologies are beginning to shape nephrology practice.
NephMadness 2026 is officially underway! The free, CME-granting, evidence-based tournament (inspired by March Madness) pits top nephrology topics against each other, from IgA nephropathy (B-cell targets vs complement inhibitors) to AI (computational pathology vs NLP) and transplantation (BK vs CMV). This year features eight regions with two subtopics each, blending serious science with creative flair. Brackets are due by March 31 at 3pm ET. Submit your picks here. (H/t Kenar Jhaveri)


ADVOCACY / SYSTEM VOICES
In Health Affairs, Dr. Suzanne Watnick argues that U.S. dialysis has become an “innovation desert” despite being uniquely positioned for research. Nearly 500,000 patients receive highly standardized, data-rich care, yet core treatment protocols have changed little since the 1980s, shaped in part by Medicare’s bundled payment system and industry consolidation, with two for-profit companies controlling ~80% of the market. Although kidney disease costs the federal government more than $150 billion annually, it receives less than 2% of NIH funding, limiting transformative research. She calls for congressional and CMS action to realign incentives, including broader value-based payment models across CKD and transplant, financial incentives for research participation, regulatory support for pragmatic trials, modernization of dialysis IT infrastructure, and reimbursement pathways that explicitly reward innovation rather than cost neutrality.
ASN’s #LoveYourKidneys campaign ramps up national media push. ASN President Samir Parikh and the ASN team recently wrapped a 17-interview satellite media tour spanning local and national outlets, including CBS News Radio, CNN Newsource, and iHeartRadio, to promote kidney health awareness ahead of National Kidney Month. The campaign bridges the transition from American Heart Month and aims to elevate public understanding of kidney disease risk, prevention, and early detection. Great work Samir, Christine, Tony and Zach— let us know if you’ve seen the message in your local area!
ASSENT launches push to validate surrogate endpoints in Alport syndrome.
The Alport Syndrome Foundation’s ASSENT Initiative (Alport Syndrome Surrogate Endpoint Network) is building an international effort to establish evidence-based surrogate endpoints to accelerate clinical trials in rare kidney diseases. Led by a multidisciplinary steering committee, including Committee Co-Chair Dr. Alex Chang, ASSENT brings together patients, regulators, nephrologists, statisticians, and global datasets to evaluate markers such as proteinuria and eGFR as trial endpoints. With multiple rare kidney trials underway across Alport syndrome, ADPKD, IgA nephropathy, AMKD, FSGS, and C3G, now is the time to shorten timelines and strengthen the path to approval for targeted therapies!Viet Le calls for unified CKM care, not siloed disease management. In his recent LinkedIn perspective, Viet Le shares that cardiovascular-kidney-metabolic (CKM) syndrome now affects ~90% of U.S. adults, yet we continue to treat A1c, eGFR, and LDL-C in isolation. He lays out a practical framework for staging CKM 0–4, aligning therapy early, and using cross-organ pillars including RAS inhibition, SGLT2 inhibitors, nonsteroidal MRAs, and GLP-1 therapies. The core message: CKM is a shared disease state, and fragmented care is the real risk factor.
TRANSPLANT STORIES
Former Bengals All-Pro Willie Anderson underwent a successful kidney transplant this month, with his longtime girlfriend serving as his living donor.
Alex Berrios received a kidney transplant in New York City this month and is now recovering post-surgery (post). After years on dialysis, he shared updates from the hospital and thanked his family for supporting him through the first days of recovery.
Ben Street, a kidney advocate and OPO leader in San Diego, is seeking a living kidney donor as his kidney function declines to 9% (post). Ben works with UCSD’s Lifesharing and serves as a National Kidney Foundation Region 9 leader, and is asking the community to share his story to help find the right donor match. Apply to be Ben’s donor here.
Events Calendar
Kidney Cancer Patient Summit, March 15 / San Diego, CA
CKD Drug Development Summit, March 16-18 / Boston, MA
LSI USA ‘26, March 16-20 / Dana Point, CA
RPA Annual Meeting, Apr 16-19 / Atlanta, GA
ANNA National Symposium, April 25-28 / New Orleans
Columbia CKM: Evolving Frontiers May 1 / Virtual
NKF Spring Clinical Meetings, May 6-10 / New Orleans
NephCure Support Groups (Ongoing)
Jobs
Nephrologist (Miami, FL) — Kaüna (Say hello!)
Manager, State Government Affairs — Takeda
Director, Partner Success — Strive Health
Sr Analyst, Medical Economics — Monogram Health
Senior Product Manager, Clinical AI — CVS Health
Director, Alliance Management — Ardelyx
Organ Health Specialist (Albany) — Natera
Sr. Medical Director (Nephrology) — Travere
Director, Donor Recovery — Donor Network of AZ
Early Pipeline Forecasting — Vertex
Analytics Technical Product Manager — Aledade
Health AI Product Manager — UC San Diego Health
Director of People — Avo
Globalization Product Manager — Getinge
…plus hundreds more at jobs.signalsfs.com
Work with us

Signals Group is expanding to support the growth of this community. Whether you’re looking to increase awareness for your work, prepare for your next milestone, or looking to enter a new market, we’d love to hear from you. We support mission-aligned organizations advancing kidney health.
Learn — Discover hundreds of articles & interviews in our Data Room
Share — See how Signals can help you reach your next milestones
Sponsor — Apply to share your mission with a kidney-focused audience
If something in this month’s recap sparked a thought, question, or you just want to learn more, hit reply. We read every note. Thanks for being here.
This audio summary may include variations in pronunciation and is intended for informational purposes only. For complete accuracy and source attribution, please refer directly to the original written materials and cited sources. Always consult trusted references when interpreting medical or scientific content.
No purchase necessary. Entry is free. Open to U.S. residents 18+. One entry per person. Ten winners will be selected at random and notified by email in April. Prizes will be delivered digitally via Tremendous, allowing winners to select from thousands of global gift card and prepaid reward options.

